Fast, Gentle Treatment of Tongue-Ties and Lip-Ties for Infants
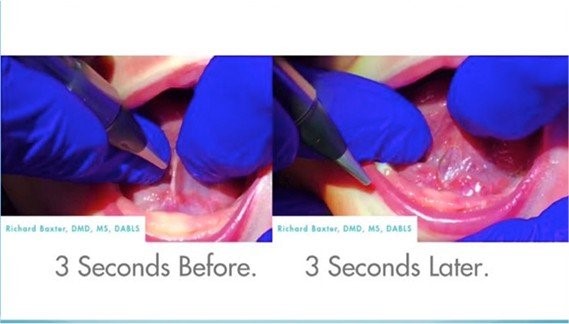
At Arlington Smile Center, Dr. Roca offers tongue-tie and lip-tie treatment for infants, using a LightScalpel® CO2 laser to sever this tight tissue with little to no bleeding and little to no pain. The procedure can be performed for a baby as young as two days old. On infants, it takes a maximum of only 15 seconds for lip-ties and eight seconds for a tongue-tie.
Treating these babies has become the most rewarding part of being a dentist for Dr. Roca. Her favorite part is listening to the change and emotion in the new mom’s experience from before the procedure to after and seeing a full, happy baby. Dr. Roca is very passionate about this topic, since she is the mom of two tongue-tied children and remembers all the struggles she faced with nursing. She wishes today’s research was available back when her kids were born. “Knowing what I know,” she says, “I would have given my right arm to have taken my kids right out of the hospital if this CO2 laser existed when my kids were born.”
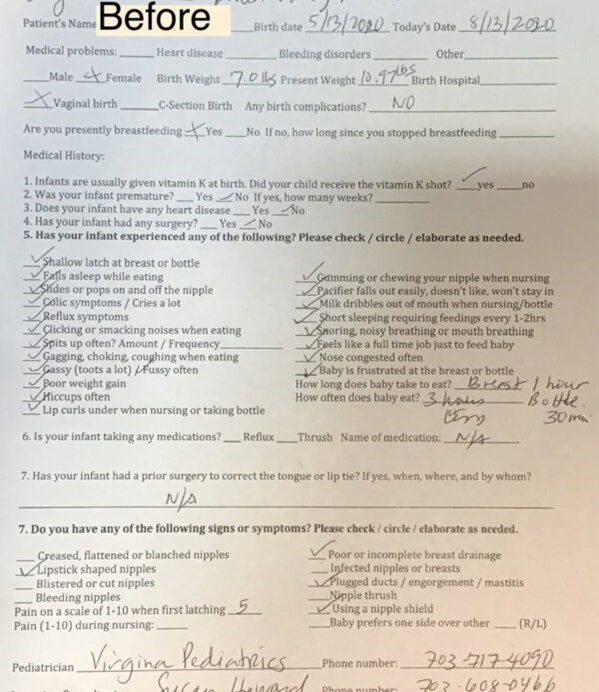
3-month-old baby — See how many check marks mom and baby were feeling
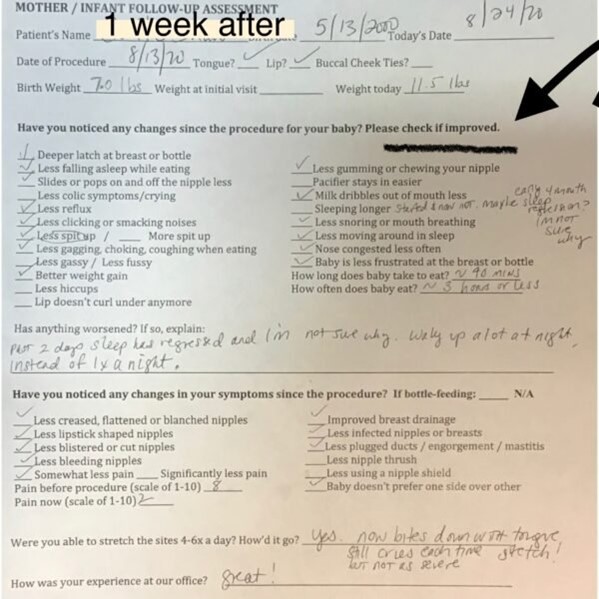
See how many check marks improved in just one week for mom and baby
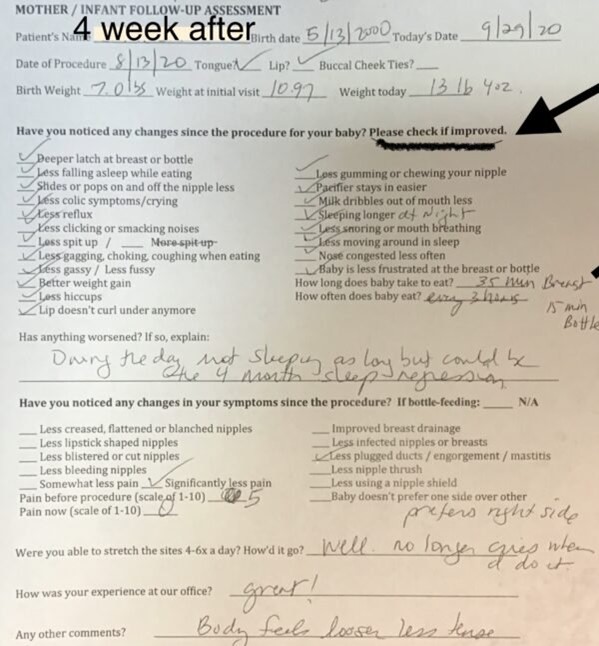
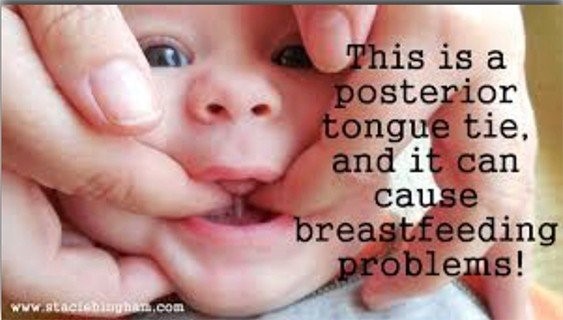
Four weeks post release and all these symptoms are better. The mother took the baby to three different consultations, where all of the doctors said there was no tie. It was a posterior tongue tie which couldn’t be seen.



(source: Darick Nordstrom/ALF and Dianah Davidson, RDH Myofunctional Therapist)
Dr. Soroush Zaghi at The Breathe Institute
One of Dr. Roca’s 5 month old patients getting a stretch day after release at home by mom. Stretch for parents should be done 6X a day for 4 weeks.
Dr. Lupita Roca is showing mom how to do the stretches on Baby M before release.
Dr. Roca finds it easier if you come from behind, and explains it is not so much a quantity of stretches as quality. Often a nice firm tug is all you need to get it done.
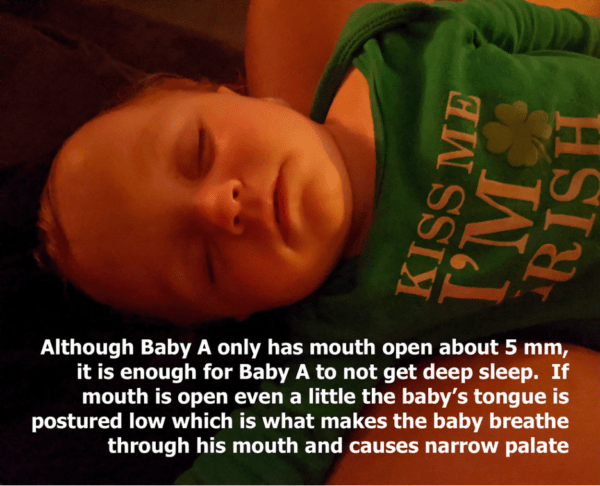
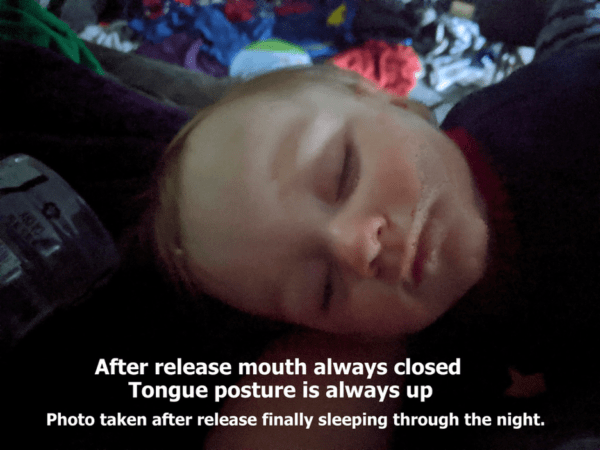
Dr. Lupita Roca gives the parents a Liper™ device, which is a tool to stretch babies after release. It really helps to get a grip on the tongue. In this video, Dr. Roca’s patient is doing an excellent job showing how to use the device with a wooden spoon she has used to prop open the mouth. She knows that Baby A does not like it, but knows it is well worth the wait. He is already sleeping better and longer without waking, without his mouth open and without snoring.
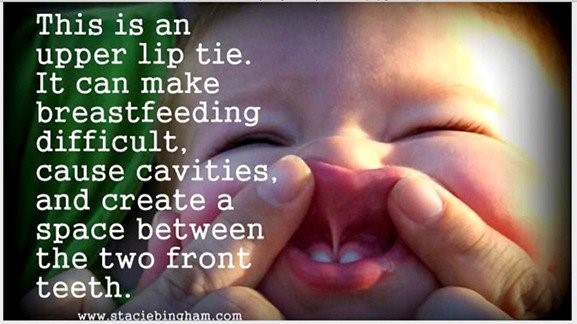
What exactly is a tongue-tie?
The lingual frenulum is a small fold of mucous membrane that extends from the floor of the mouth to the midline of the underside of the tongue. Find your own lingual frenulum by looking in the mirror, opening your mouth, and stretching your tongue towards the palate. See the whitish cord beneath your tongue? Ankyloglossia, or tongue-tie, is simply a lingual frenulum that is tight enough to restrict the movement of the tongue. It is a congenital oral anomaly caused by an unusually thick, or unusually short, lingual frenulum.
Can a tongue-tied baby stick her tongue out past her lips?
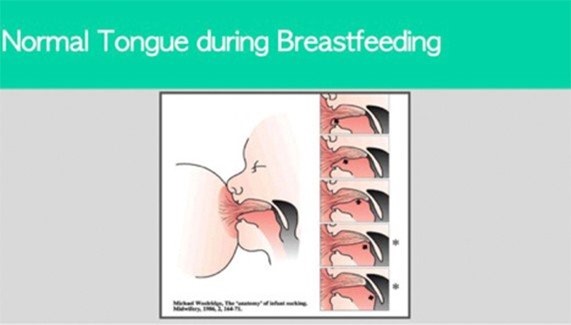
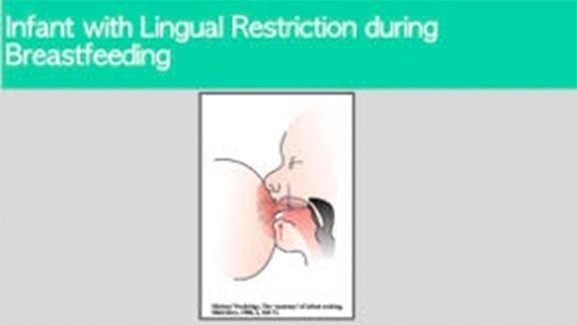
Absolutely. Just because the tongue has normal motion in one direction doesn’t mean it has normal motion in all directions. The most important movement for the tongue during breastfeeding is up and not out, so the normal outward movement of the tongue is as relevant as normal shoulder movement for the purposes of breastfeeding.
My baby’s tie has been cut. Why is her tongue still heart-shaped?
The band that had tethered the tongue to the floor of the mouth travels from within the substance of the tongue down to the floor of the mouth. Cutting that band somewhere in the middle doesn’t remove the portion of the band inside the tongue. It can still change the shape of the tongue, but typically doesn’t affect function.
I have no difficulties with breastfeeding, but it looks like my baby has a tongue-tie. What should I do?
Dr. Roca, herself, thought she had no trouble with breastfeeding. In fact, she thought her son loved to breastfeed, but now she knows that the reason he wanted to nurse all the time was because he was never full, which would explain why he would start to cry as soon as he was put into his crib. He was still hungry, so he would tire himself out trying to obtain enough milk, and as soon as they went to put him down, he would wake up and want to nurse again. The moral of the story is that even if your baby is nursing fine and gaining weight, it would still be worth looking into releasing the tongue-tie, because the tongue-tie will lead to more serious health issues as an adult.
Can you describe the procedure on a baby that is tongue-tied? Does it hurt?
The infant frenectomy is a straightforward outpatient procedure that can be completed during the same visit as the initial assessment. If a release is recommended, the treatment takes only a few minutes, and a baby can go to the breast immediately following. The baby is swaddled and safety goggles are always used to protect baby’s eyes. Dr. Roca uses a pen-sized laser on infants to remove the tight lingual frenulum. She applies an effective topical anesthetic gel on the frenular tissue prior to treatment, allowing for zero to minimal discomfort during the procedure. The anesthetic lasts for approximately 30 minutes.
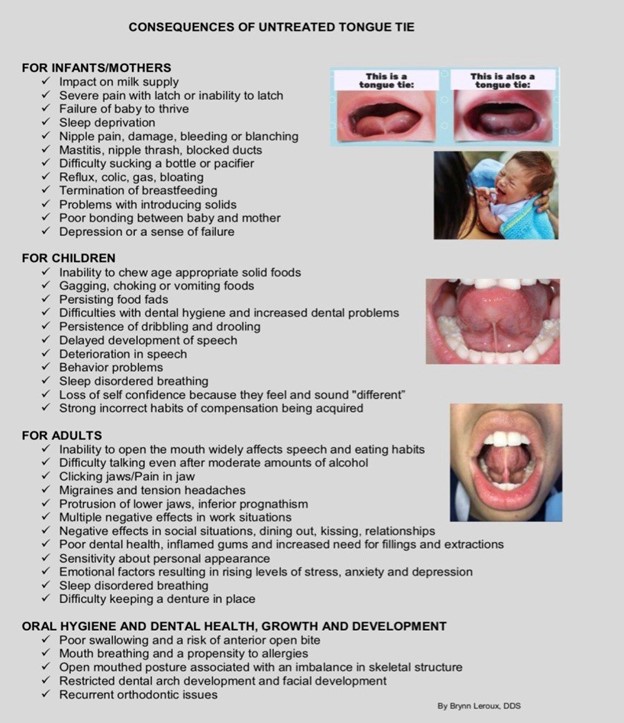
What type of issues do mothers of breastfeeding infants experience?
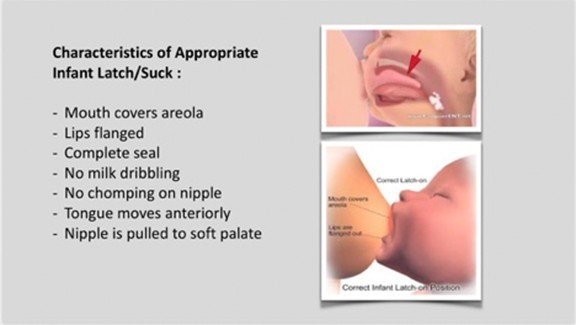
Studies have shown that an infant with tongue-tie can have issues latching, gaining weight, creating suction and staying awake during feeding due to the extra exertion required. In addition, mothers with infants who are tongue-tied may experience significant pain in their nipples, to the extent that they can become cracked and abscessed. If symptoms including inadequate latch, poor breast draining, painful nipples, and/or fussiness at the breast have not improved and a lactation consultant is concerned about a possible tongue-tie, she will refer mom and baby. Babies are smart — over the weeks, they figure out what to do to survive and make compensations. Mothers think they are nursing great, but if the mother needs to supplement, or if the baby eats like the mom is a snack bar and doesn’t want to fall asleep for a long period, the baby may appear to be nursing fully but is not able to fill out so will be looking for the breast repeatedly.
How do you correspond with lactation consultants before and after treatment?
Dr. Roca’s goal during the first visit is to gather as much information as she can about the specific breastfeeding issues mom is facing. Therefore, prior to an initial consultation appointment, she will be in contact with the lactation consultant working with mom and baby in order to gain background knowledge on their sessions together. This allows us to work together to best gauge a baby’s progress in nursing. Dr. Roca works with a number of reputable lactation consultants in our community who are comfortable in assessing oral restrictions. When communicating with moms pre-treatment, we cannot stress enough the importance of continued lactation support following the frenectomy procedure.
What can you expect to happen after the procedure?
Breastfeeding is encouraged immediately following the procedure while still in our office. However, typically there is a healing period that your infant must undergo before the full benefits are realized. Mothers are always thrilled right after they nurse, and we tell them it will only get better if they keep up with full stretches. We teach each mother proper active wound management and daily stretching exercises in order to facilitate healing. We cannot stress enough the importance of continued lactation support following the frenectomy procedure. Post-treatment follow-up is just as important as pre-treatment care. Dr. Roca sends a detailed report of her assessment and/or procedure to the lactation consultant and stays up to date with baby’s progress after our four-day follow up. Baby will continue to build strength over the healing period and will require further guidance on developing positive breastfeeding habits. It is not only the tongue and jaw that prove to be key components in breastfeeding, but, in fact, the whole body.
For this reason, tongue-tied babies often have additional structural stressors to be addressed and we will recommend taking baby to see a bodyworker, a licensed professional such as an occupational, craniosacral or physical therapist. Bodywork encourages body awareness and encourages an infant to express postural reflexes and explore natural movement inclinations through the nervous system. After a tongue-tie release, the infant’s tongue will need to adapt to a new and profound range of motion. Often while in utero, the babies develop wry neck, or torticollis, which is a painfully twisted and tilted neck. The top of the head generally tilts to one side while the chin tilts to the other side. This condition can be congenital (present at birth) or acquired. It can also be the result of damage to the neck muscles or blood supply. Wry neck sometimes goes away without treatment, but often, we can tell an infant has torticollis because they prefer one breast to the other or their neck is very tight. This is an example where we would refer your baby for some body work.
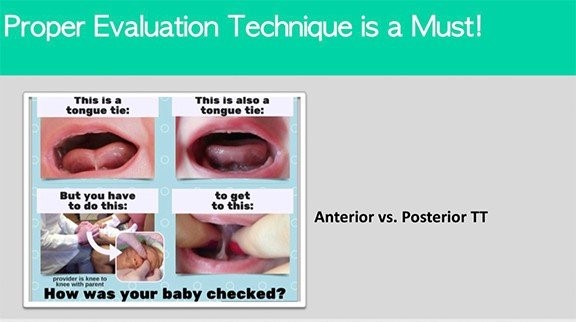
At the hospital, my baby was checked for tongue- and lip-tie and they said he was fine. But in my gut, I know it’s not right. Can we bring the baby in for a quick second opinion?
Yes, we would love to meet your baby for a quick visit. Dr. Roca would even come out to the parking lot to take a quick peek, or you could send her a photo. It is always best to be sure. Mothers always know best — even new moms!
My baby’s tongue-tie was released before, but I don’t think it was released enough. Is it possible that the child needs the tongue-tie released again?
Yes, often we release tongue-ties on children that have been released as many as four times. Scar tissue can grow back if not stretched correctly post-op and for the weeks following the release. Arlington Smile Center sees all releases one week post-op to make sure the membrane is not starting to reattach.
My baby is nursing fine and growing more every day. I don’t want to put my infant through a tongue-tie release if life is good.
Dr. Roca completely agrees. If your baby is feeding every three hours during the day, you are sleeping all night and baby settles easily without waking, enjoy your baby. However, please note that if a posterior tongue-tie or anterior tongue-tie exists, you want to make sure it is released as a toddler to have the best chance to avoid an airway breathing disorder and unnecessary compensations that will lead to medical concerns.
In Dr. Roca’s clinical experience, even if your child is 2+ years old and has immature gag reflex, are struggling with chewing “hard solids”, mouth breathing, etc., starting with chewy tube and age appropriate myofunctional therapy exercises along with encouraging parents to familiarize themselves with improving gut health and body work have proven to be the most successful and stress-free way for parents to help their children develop correct oral mouth posture and nose breathing.
Below are great books to help with these next step for your babies.
No one needs to live with the difficulties of tongue-ties and lip-ties. Call 703-237-7622 now to schedule a visit to see how we can help you or your child.