What is a miniscrew-assisted rapid palatal expansion (MARPE)?
Certain aspects of obstructive sleep apnea, such as nasal blockage, impeded facial development and teeth that are crowded together, are connected with having a narrow maxilla, or upper jaw. MARPE expands the maxilla effectively. This method does not require surgery or tooth extractions.The typical maxillary expanders for a narrow maxilla are limited to children. This is due to the fact that the suture that holds the maxillary bone together, also known as the midpalatal suture, usually fuses when children are between 12-15 years old. However, MARPE can be used for a wider age range since it connects the expander to the palatal bone, helping adults that already have a fused suture. MARPE can also help children that experience sleep problems.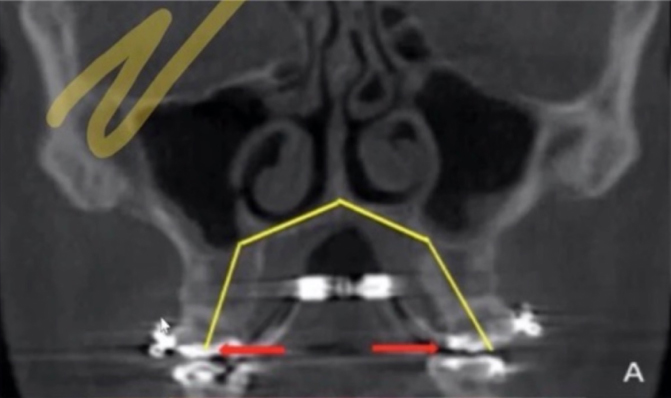


Courtesy of Dr. Audrey Yoon
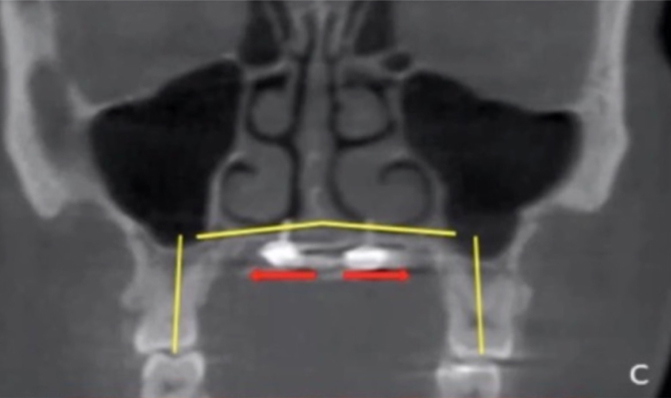
Photos A and B above show dental expansion through fixed expanders, whereas photos C and D above are showing skeletal expansion assisted by micro-implants (miniscrews). The difference between the two is that dental expansion is moving teeth while skeletal expansion is opening up the bone. Skeletal expansion is much more permanent due to the bone filling in, whereas in dental expansion, the teeth can move back and the palate become narrow again.
M
Miniscrew
A
Assisted
R
Rapid
P
Palatal
E
Expansion
MSE = Maxillary Skeletal Expansion which is a type of MARPE
Start of expansion with MSE

One month later, you can see space between the two front teeth


Finished expansion. She could have had her jaw expanded more, but we had the expansion we needed to fit her tongue
How does MARPE operate?
Why MARPE?
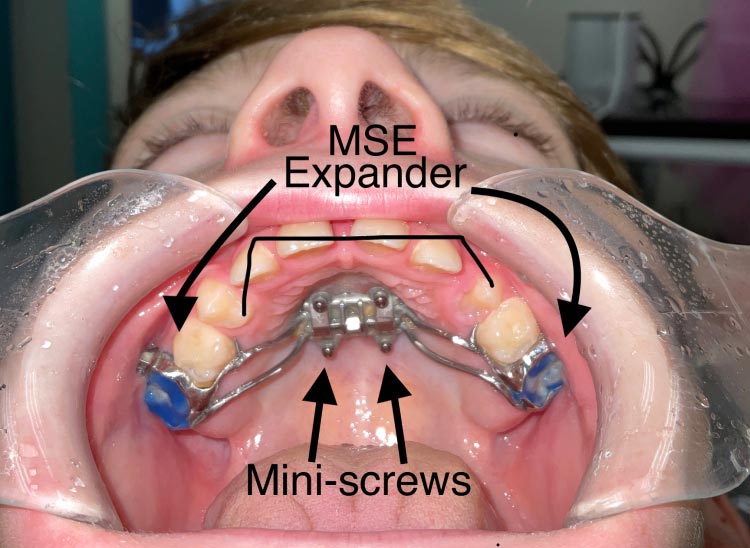
The photo above is an example of an MSE MARPE.
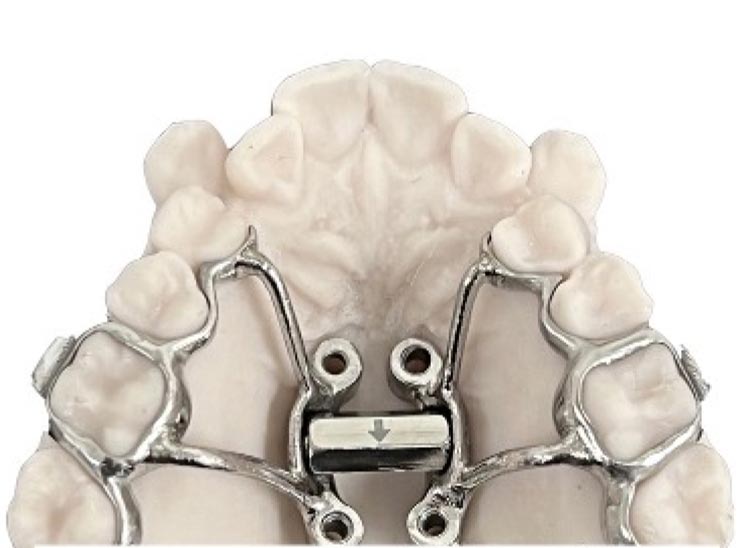
The photo above is an example of the type of MARPE we use for small mouths that would be too small for an MSE. It uses a Super Screw that allows for even better results. It is also easier for patients to turn.
Why Us?
Why would the patient want the MARPE (miniscrew-assisted rapid palatal expander) placed by Dr. Roca at Arlington Smile Center vs. other offices?- Every patient gets a custom MARPE (miniscrew-assisted rapid palatal expander). Dr. Roca sends the patient’s 3D CBCT X-rays to the lab along with an iTero® scan of the patient’s teeth, and she meets with the lab over Zoom to discuss each MARPE case. The lab marries the two images in order to determine the best location for the miniscrew and determine what length is needed according to the thickness of bone. Everyone is different, so we found just placing an MSE was not good enough. We might use MSE, but it will be a custom MSE, often with more than 4 TADs.
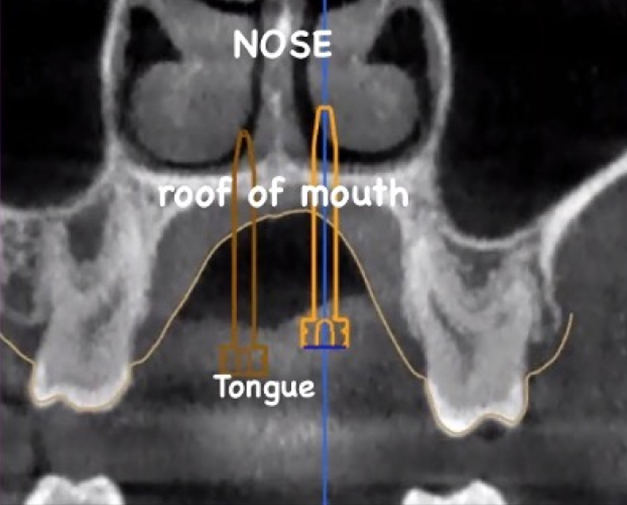
The X-ray above is the view looking at the nose. The screws are on either side of the septum.
Miniscrews are 8 mm to 17 mm, depending on the thickness of the bone.
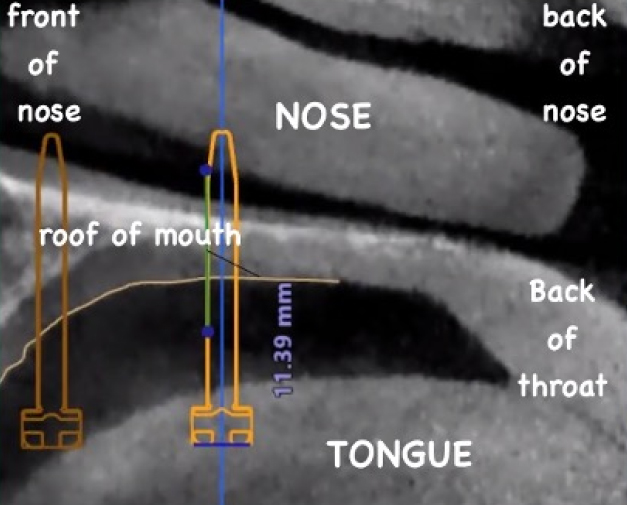
The X-ray above is looking at the side of the face. Micro-implants appear much larger than they are in the mouth. We merge the X-ray and the scan of the teeth into one image to get the exact ideal location for the micro-implant placement. We are looking for the location of the best bone available for insertion.
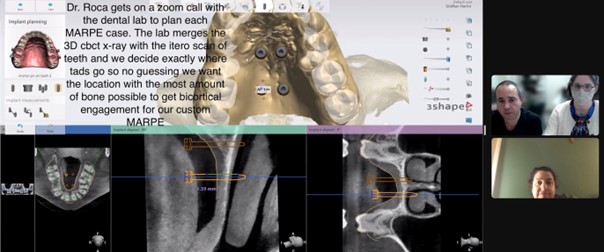
As shown by the photo above, Dr. Roca gets on a Zoom call with the dental lab to plan each MARPE case. The lab merges the 3D CBCT X-ray with the iTero scan of the teeth and decides exactly where the TADs go, so there is no guessing. We want the location with the most amount of bone possible to get bicortical engagement for our custom MARPE.
- Every patient gets a custom MARPE (miniscrew-assisted rapid palatal expander). Dr. Roca sends the patient’s 3D CBCT X-rays to the lab along with an iTero® scan of the patient’s teeth, and she meets with the lab over Zoom to discuss each MARPE case. The lab marries the two images in order to determine the best location for the miniscrew and determine what length is needed according to the thickness of bone. Everyone is different, so we found just placing an MSE was not good enough. We might use MSE, but it will be a custom MSE, often with more than 4 TADs.
- Dr. Roca has spent many hours learning from Postural Restoration Institute® (PRI). All our MARPE patients are encouraged to work with one of two physical therapists in the area that understand the need for the body to be neutral. They have been trained by the Postural Restoration Institute school of thought. The concept is that when the patient is locked head down, it is often due to the bite not allowing the neck and body to be neutral due to the temporal bones and sphenoid being locked into position, creating the asymmetrical expansion. We want to achieve symmetrical expansion on all cases. We determine if the neck is neutral by referring them to these specific physical therapists that follow the patient through treatment. Dr. Roca already has an idea that patients are not neutral when she sees one shoulder taller, or a neck tilted to one side, or one ear tucked back, one eye higher or a forward head posture.The key is that the temporal bones on both sides of the head need to move with each step we take and that the sphenoid bone that is located behind the eyes and connected to both temporal bones cannot be locked in place. Otherwise, the side of the palate that was more expanded to begin with continues to expand more than the side that needs the most expansion. One of the easiest ways we can make sure if you are neutral is checking your breathing and seeing if changing the bite influences the amount of air and noise that you are able to emit through your nostril. Arlington Smile Center is committed to keeping you neutral during our expansion cases, and we have many ways to do so that we will share during your consult.
- Dr. Roca has spent many hours learning from Postural Restoration Institute® (PRI). All our MARPE patients are encouraged to work with one of two physical therapists in the area that understand the need for the body to be neutral. They have been trained by the Postural Restoration Institute school of thought. The concept is that when the patient is locked head down, it is often due to the bite not allowing the neck and body to be neutral due to the temporal bones and sphenoid being locked into position, creating the asymmetrical expansion. We want to achieve symmetrical expansion on all cases. We determine if the neck is neutral by referring them to these specific physical therapists that follow the patient through treatment. Dr. Roca already has an idea that patients are not neutral when she sees one shoulder taller, or a neck tilted to one side, or one ear tucked back, one eye higher or a forward head posture.The key is that the temporal bones on both sides of the head need to move with each step we take and that the sphenoid bone that is located behind the eyes and connected to both temporal bones cannot be locked in place. Otherwise, the side of the palate that was more expanded to begin with continues to expand more than the side that needs the most expansion. One of the easiest ways we can make sure if you are neutral is checking your breathing and seeing if changing the bite influences the amount of air and noise that you are able to emit through your nostril. Arlington Smile Center is committed to keeping you neutral during our expansion cases, and we have many ways to do so that we will share during your consult.
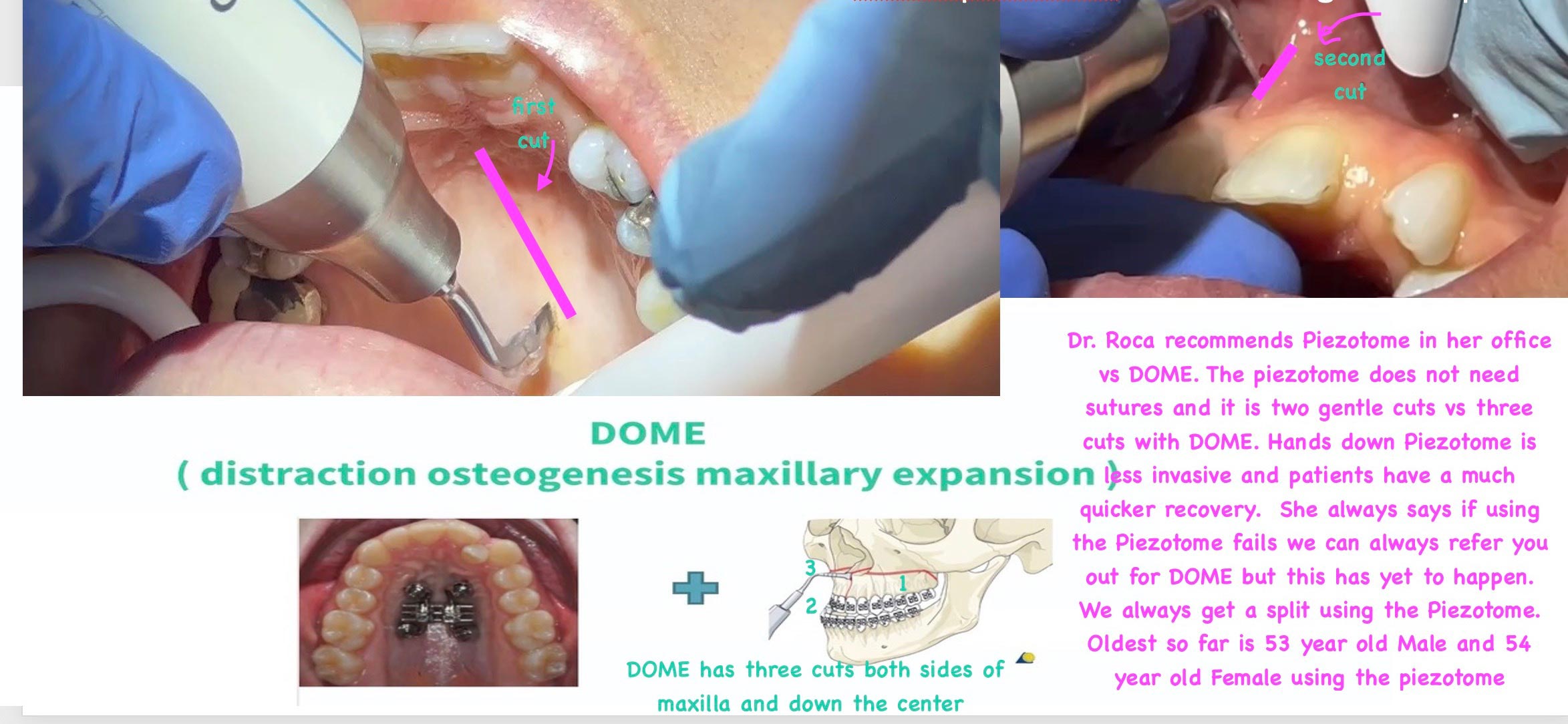
- In the past, adults that had a narrow upper jaw and bite problems needed to undergo surgically-assisted rapid palatal expansion (SARPE). SARPE is an invasive procedure that, like distraction osteogenesis maxillary expansion (DOME), corrects narrow plates. However, at Arlington Smile Center, Dr. Roca uses a Piezotome® CUBE to make two cuts in the suture to give the palate a head start in splitting. We do this for all male patients that are over 25 and female patients 35 or older. This is a specialized procedure taught to Dr. Roca by Dr. Ilya Lipkinm, a well-known orthodontist in New Jersey who has placed over 1,000 MARPE appliances successfully with minimal failures.We have found Piezotome® CUBE so much easier for the patient and more comfortable than corticopuncture.For all men over 25 and all women 35 and older, we highly recommend the use of the Piezotome CUBE instead of corticopuncture, due to its predictability. Dr. Roca learned this technique from Dr. Lipkin and Dr. Ting. So far, the doctor’s oldest male patient is 53 and the oldest female patient is 54. This has increased our predictability immensely.
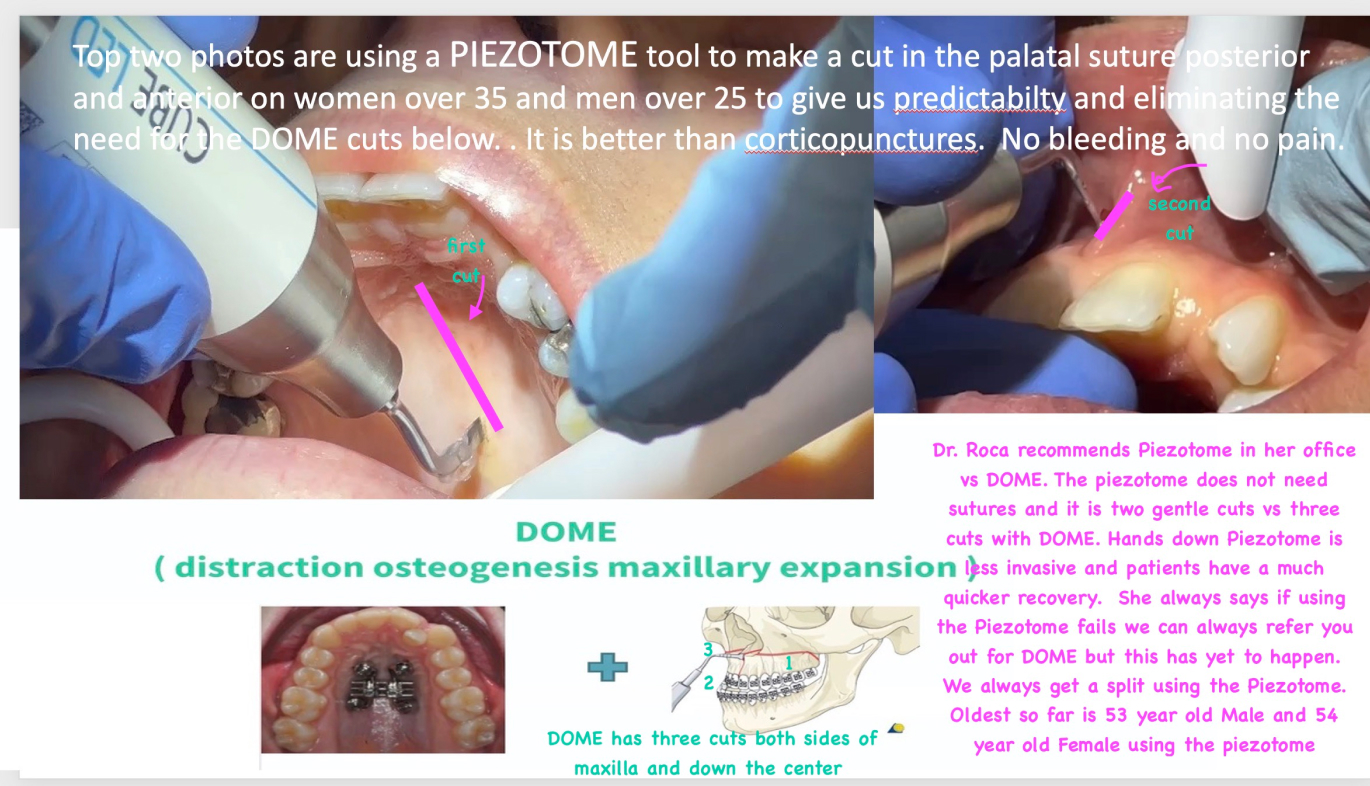
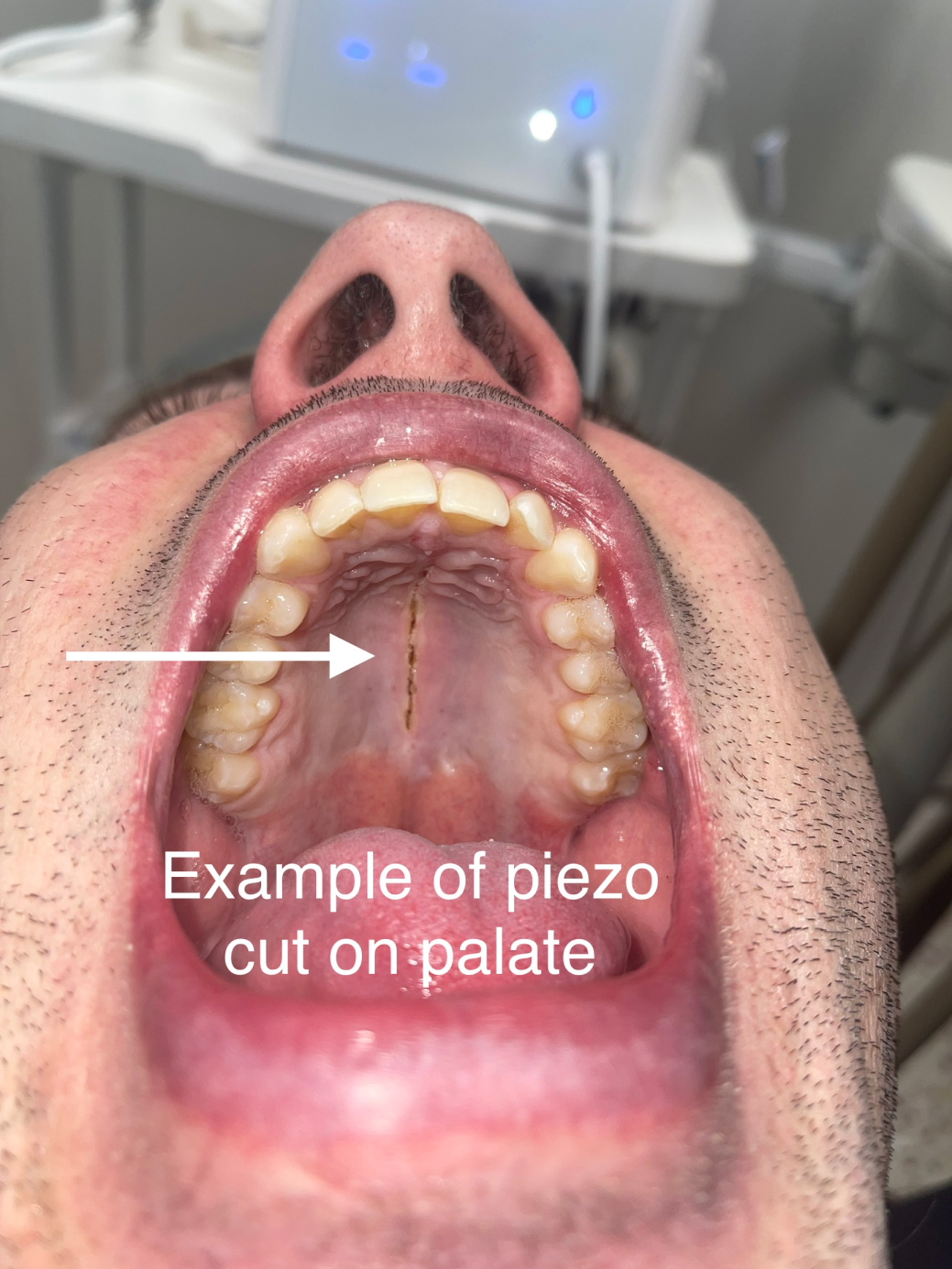
In the top two photos, Piezotome CUBE is being used to make a cut in the palatal suture posterior and anterior. We use this tool on women over 35 and men over 25 to give us predictability and eliminate the need for the DOME cuts below. It is better than corticopuncture. There is no bleeding and no pain.
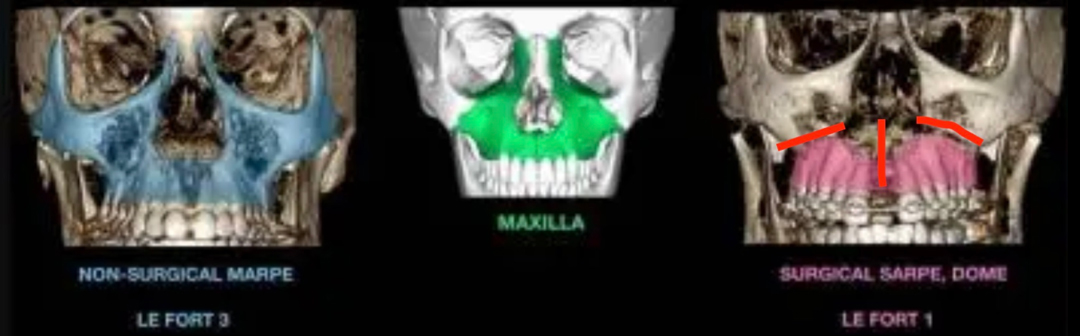
The slide above is one Dr. Roca borrowed from Dr. Marianna Evans’ lecture that does a great job of explaining the difference between different procedures. The reasons that Dr. Roca prefers using a Piezotome CUBE versus referring patients out for DOME or SARPE are that it allows for a much quicker recovery, does not require patients to go the hospital for procedure and allows for the zygoma to widen as well.
- In the past, adults that had a narrow upper jaw and bite problems needed to undergo surgically-assisted rapid palatal expansion (SARPE). SARPE is an invasive procedure that, like distraction osteogenesis maxillary expansion (DOME), corrects narrow plates. However, at Arlington Smile Center, Dr. Roca uses a Piezotome® CUBE to make two cuts in the suture to give the palate a head start in splitting. We do this for all male patients that are over 25 and female patients 35 or older. This is a specialized procedure taught to Dr. Roca by Dr. Ilya Lipkinm, a well-known orthodontist in New Jersey who has placed over 1,000 MARPE appliances successfully with minimal failures.We have found Piezotome® CUBE so much easier for the patient and more comfortable than corticopuncture.For all men over 25 and all women 35 and older, we highly recommend the use of the Piezotome CUBE instead of corticopuncture, due to its predictability. Dr. Roca learned this technique from Dr. Lipkin and Dr. Ting. So far, the doctor’s oldest male patient is 53 and the oldest female patient is 54. This has increased our predictability immensely.
- Patients that get MARPE from Dr. Roca at Arlington Smile Center are given her personal cell phone number and asked to text photos every Sunday so she can confirm that the expansion is happening symmetrically and the patient is following directions. She looks at these photos closely every week to follow each case and make sure we do not need to pause or change course.
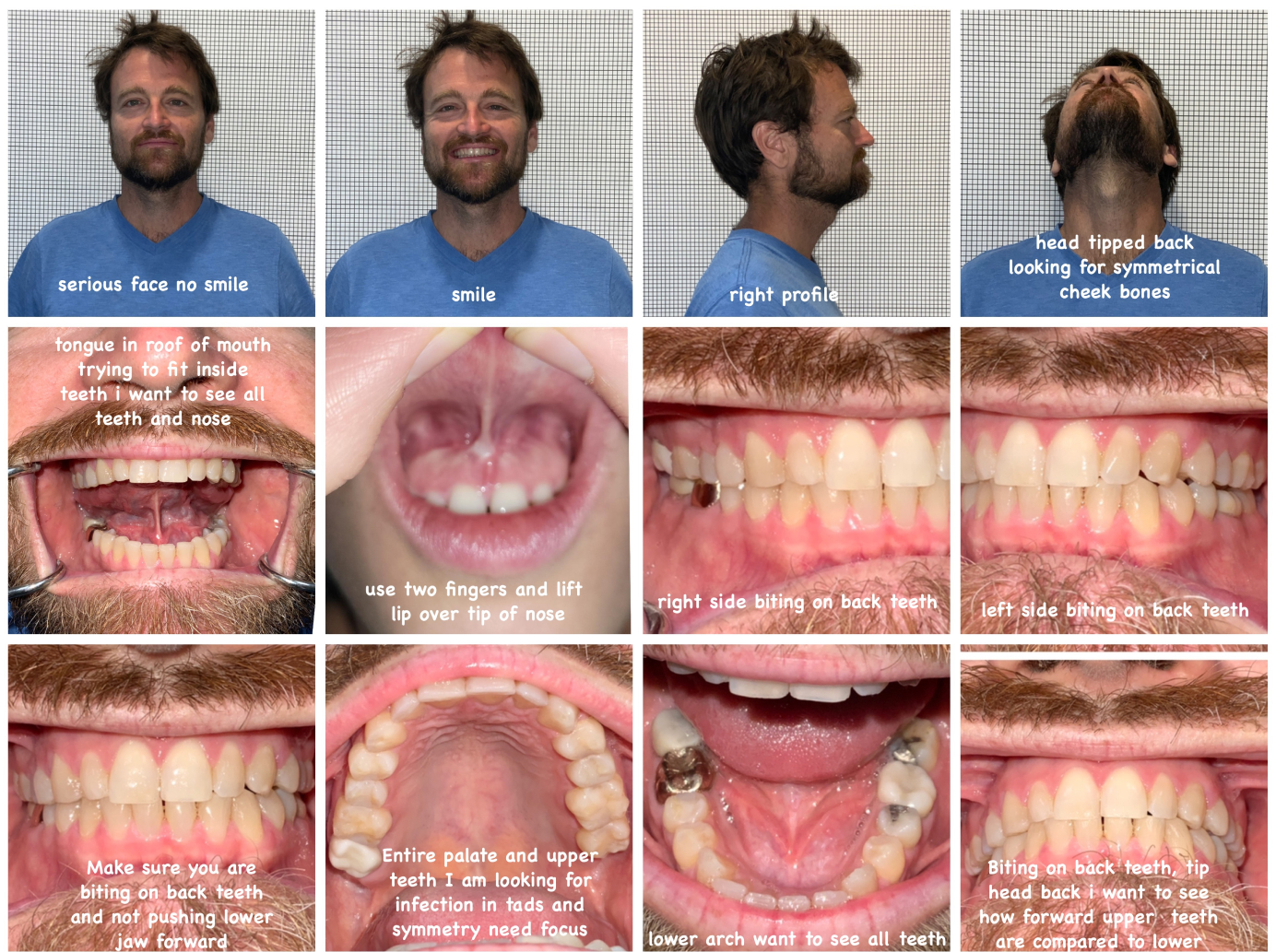 Please send these photos to Dr. Roca every Sunday, as it is her least busy day. Please send early in the day if possible. Please have someone take your photos if you can or use a bathroom mirror. Dr. Roca is looking for infection under the lip, so she needs the lip pulled way over the nose if possible. Dr. Roca is looking for infection and that the expansion is as symmetrical as possible. Please use the flash for all of the photos. You will need to make sure the flash is turned on each time and that the photo is in focus. If you wet plastic before putting it in the mouth, it works easier. Ideally, there should be less facial hair when possible, and you should have your hair behind your ears and not be wearing glasses. Use a blank wall.
Please send these photos to Dr. Roca every Sunday, as it is her least busy day. Please send early in the day if possible. Please have someone take your photos if you can or use a bathroom mirror. Dr. Roca is looking for infection under the lip, so she needs the lip pulled way over the nose if possible. Dr. Roca is looking for infection and that the expansion is as symmetrical as possible. Please use the flash for all of the photos. You will need to make sure the flash is turned on each time and that the photo is in focus. If you wet plastic before putting it in the mouth, it works easier. Ideally, there should be less facial hair when possible, and you should have your hair behind your ears and not be wearing glasses. Use a blank wall.
- Patients that get MARPE from Dr. Roca at Arlington Smile Center are given her personal cell phone number and asked to text photos every Sunday so she can confirm that the expansion is happening symmetrically and the patient is following directions. She looks at these photos closely every week to follow each case and make sure we do not need to pause or change course.
- Our patients that need to correct their underbites or crossbites and have small airways are encouraged to use a reverse-pull facemask to get some anterior-posterior growth (sagittal) instead of just transverse growth.

Photos above were taken three weeks after MARPE was placed<br/ > Patient was a 36-year-old male<br/ > MARPE placed: 7/22/22<br/ > Photo date: 8/13/22

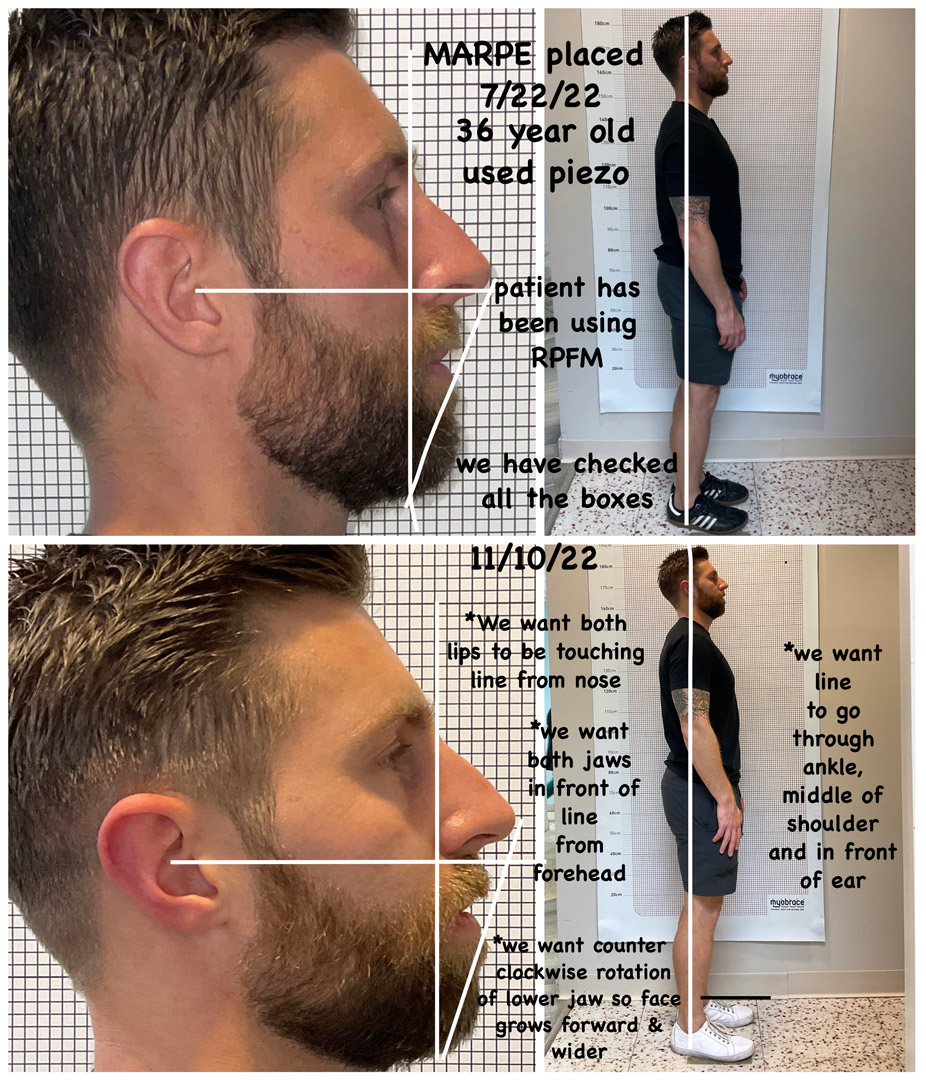
11/10/22
* We want both lips to be touching the line extending from the nose
* We want both jaws in front of the line extending from the forehead
* We want a counterclockwise rotation of the lower jaw so the face grows more forward and wider
* We want the line to go through the ankle, middle of the shoulder and in front of the ear
- Our patients that need to correct their underbites or crossbites and have small airways are encouraged to use a reverse-pull facemask to get some anterior-posterior growth (sagittal) instead of just transverse growth.
- Dr. Roca has learned techniques from Dr. Won Moon, Dr. Rebecca Brokow, Dr. Marianna Evans, Dr. Audrey Yoon, Dr. Richard Ting and, last but not least, Dr. Ilya Lipkin. Dr. Roca has found Dr. Lipkin’s protocols the best because they are gentle, custom and predictable. Dr. Roca says, “Placing MSE is so much easier than implants since no dangerous structures are in our way. Especially with our custom MARPE, there is no longer any guesswork.”
MARPE/MSE
Turning schedule following Dr. Roca’s protocol she learned from Dr. Ilya Lipkin.
For children with a narrow maxilla but no Class III malocclusion:
- After the MSE is placed, wait one week before turning twice, either at home or at our office. The MSE will then be turned once a day for three weeks.
- After three weeks of daily turning, the turning schedule can slow to a minimum of three turns a week if the child experiences discomfort or to let the lower jaw catch up. If there are no issues, keep turning daily until Dr. Roca says otherwise.
- Once the split takes place, our team will cut off the arms. The MSE will remain on for another six months after the turning ends.
For children with a narrow maxilla and a Class III bite or Class III tendency, which means they will be using a reverse-pull facemask:
- After the MSE is placed, wait one week turning twice. This will be done either at home or at the office. For the next three weeks, turn once a day.
- Patients should start using the reverse-pull facemask one week after turning has begun.
- After three weeks, start turning three times a week until Dr. Roca says the expansion is finished.
- After that time, if we need more forward growth, the patient will follow this protocol until the crossbite is corrected: For one week, turn backwards once a day. Turn forward once a day the next week, and then do not turn for a week. Then repeat the cycle with one week of backwards turns, one week of forward turns and one week of rest until the upper jaw has gone forward as much as it can go.
- The MSE’s bands will have to stay on the teeth so there is a place to attach the facemask’s rubber bands.
- Leave the MSE in place for six months after the last turn.
For adults improving sagittal airway dimensions or a Class III bite and not using a facemask:
- The day the MSE is placed, if the Piezotome CUBE was used, turn four or five times until you experience resistance. If the Piezotome CUBE was not used, turn two to four times until you experience resistance.
- Turn once every day until maxed out or the appliance fails.
- Once the expansion and protraction are finished, our team will cut off the arms. Then they will start orthodontic treatment on the upper arch and continue orthodontic treatment on the lower arch.
- The MARPE will be left in place without the arms for eight months after the expansion and protraction are complete and the turning is finished.
For adults improving sagittal airway dimensions or an anterior Class III bite and using a facemask:
- After the MSE is placed, turn four to five times until met with resistance. If the Piezotome CUBE was not used, turn two to four times until you met with resistance. Start wearing the facemask right away
- Turn once a day until the split takes place. After, turn three times a week for more forward growth with the facemask.
- If the expansion is maxed out before reaching the ideal forward growth, start turning backwards once a day for one week. The following week, turn forward once a day and then rest for a week. Restart the cycle of one week backward, one week forward and one week of rest.
- Once the expansion and protraction are finished, our team will cut off the arms and start orthodontic treatment on the upper arch, continuing orthodontic treatment on the lower arch.
- The MARPE will stay in place without the arms for eight months after the expansion and protraction are complete and the turning is complete.
- Dr. Roca has learned techniques from Dr. Won Moon, Dr. Rebecca Brokow, Dr. Marianna Evans, Dr. Audrey Yoon, Dr. Richard Ting and, last but not least, Dr. Ilya Lipkin. Dr. Roca has found Dr. Lipkin’s protocols the best because they are gentle, custom and predictable. Dr. Roca says, “Placing MSE is so much easier than implants since no dangerous structures are in our way. Especially with our custom MARPE, there is no longer any guesswork.”
- Dr. Roca uses a new feature from Invisalign® that merges the patient’s CBCT data so she knows exactly how much expansion [hehse] can get on the lower arch while keeping the teeth within the bone and avoiding the need for surgically facilitated orthodontic therapy (SFOT). See directly below a video of the CBCT data merged with the scan of the teeth.This is how Dr. Roca previously calculated how much expansion she could do to avoid SFOT. But now that Invisalign has merged the CBCT with the teeth scan, this has not become guesswork anymore.
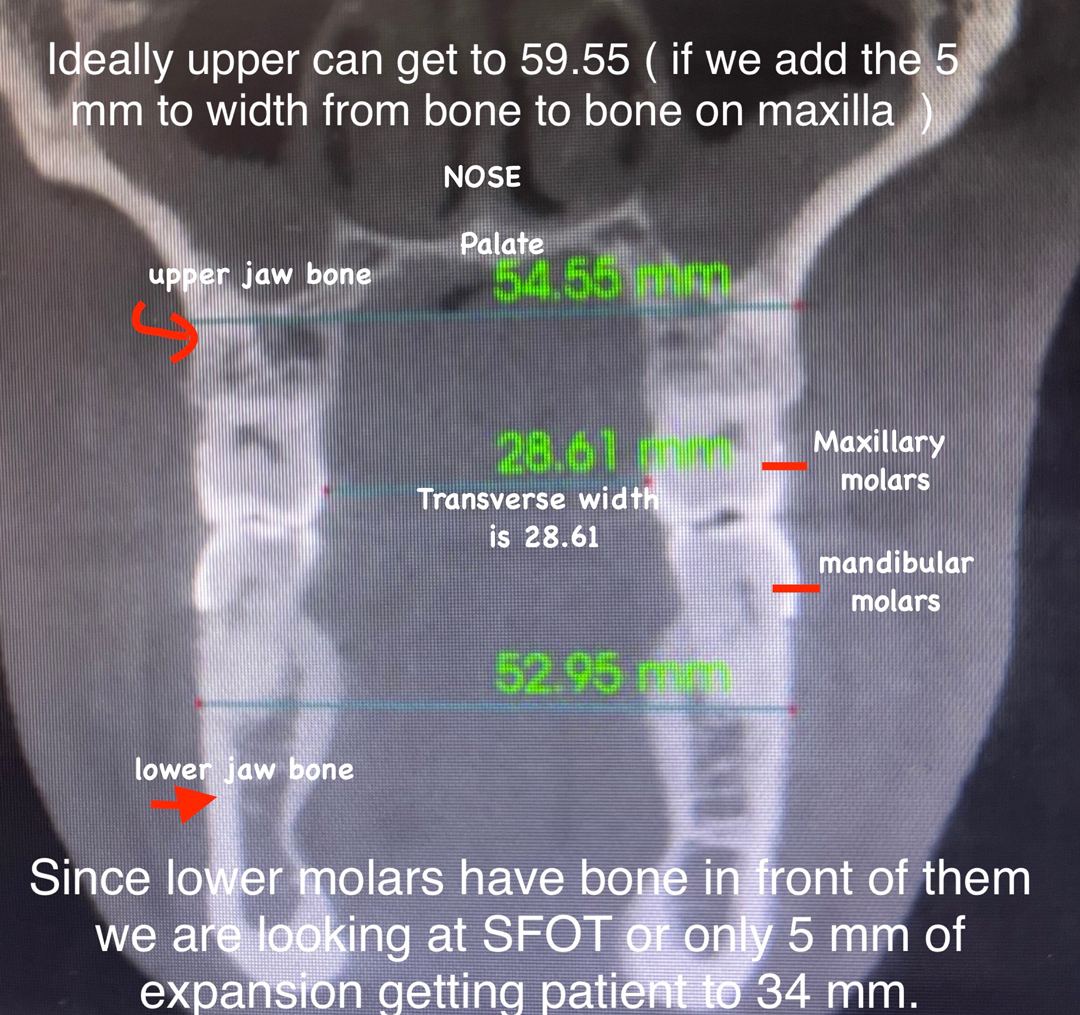
The X-ray above shows the upper and lower jawbones. Ideally, the upper palate can get to 59.55 (if we add the 5 mm to width from bone to bone on maxilla).
Since these lower molars do not have bone in front of them, we are looking at SFOT for the lower jaw or only 5 mm of expansion to get the patient to 34 mm.
An advanced procedure known as surgically facilitated orthodontic therapy (SFOT) addresses deficiencies in the alveolar bone and arch forms that have been compromised. SFOT helps to enhance the function and appearance of the smile. SFOT may be needed on the lower palate if we need more expansion on the lower palate than the current lower bone can handle. Often, we do what we can with Invisalign and MSE. If a patient has a reduced apnea-hypopnea index (AHI) score and better breathing, we do not need SFOT.
- Dr. Roca uses a new feature from Invisalign® that merges the patient’s CBCT data so she knows exactly how much expansion [hehse] can get on the lower arch while keeping the teeth within the bone and avoiding the need for surgically facilitated orthodontic therapy (SFOT). See directly below a video of the CBCT data merged with the scan of the teeth.
- Since Dr. Roca is a cosmetic dentist, she can also add some bonding material between your teeth to make the space not look so big for an additional fee.

- Since Dr. Roca is a cosmetic dentist, she can also add some bonding material between your teeth to make the space not look so big for an additional fee.
- Since Dr. Roca does all her own dentistry, we will be able to help you and follow closely the state of your teeth, health, earlier dental work and future dental work that could be needed. For example, we test the health and vitality of each tooth involved with the MARPE before we place the MARPE and track these teeth along the way. To learn more about MSE and MARPE in Arlington, Virginia, we invite you to call us at 703-237-7622 to schedule an appointment with our dentist.
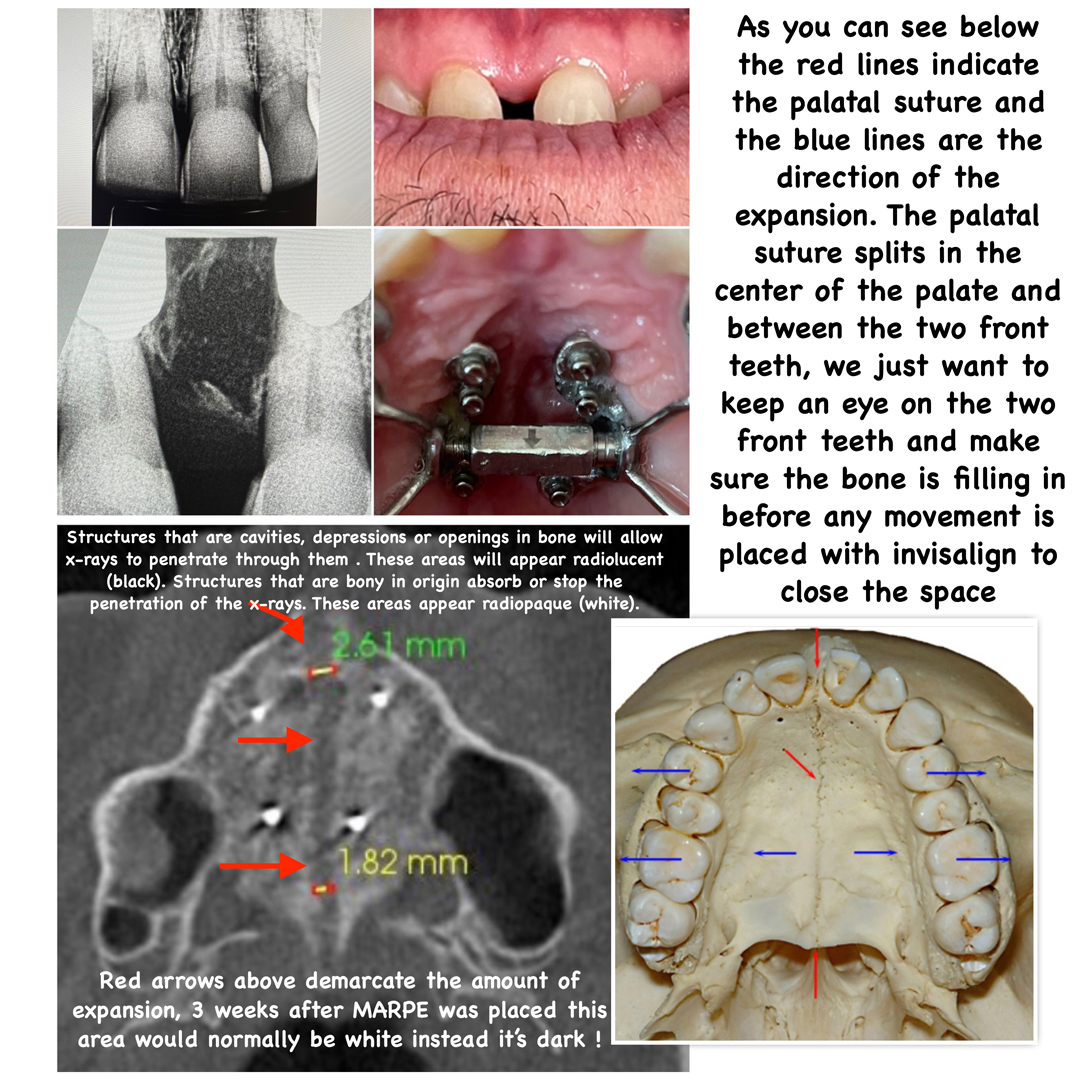
Structures that are cavities, depressions or openings in bone will allow X-rays to penetrate through them. These areas will appear radiolucent (black). Structures that are bony in origin absorb or stop the penetration of the X-rays. These areas appear radiopaque (white).
Red arrows in the bottom left X-ray above demarcate the amount of expansion. This X-ray is from three weeks after MARPE was placed. This area would normally be white, but instead it is dark!
The red lines in the bottom right picture above indicate the palatal suture, and the blue lines are the direction of the expansion. The palatal suture splits in the center of the palate and between the two front teeth. We just want to keep an eye on the two front teeth and make sure the bone is filling in before any movement is placed with Invisalign to close the space.
The collage below is of one of our patients, who is 44 years old. He was not ready for MARPE yet and wanted to start with the Homeoblock™. We did the Homeoblock for a year. It improved his sleep, body pains and breathing while sleeping, but he was not able to get the kind of expansion we wanted from the Homeoblock since his suture were so tight.
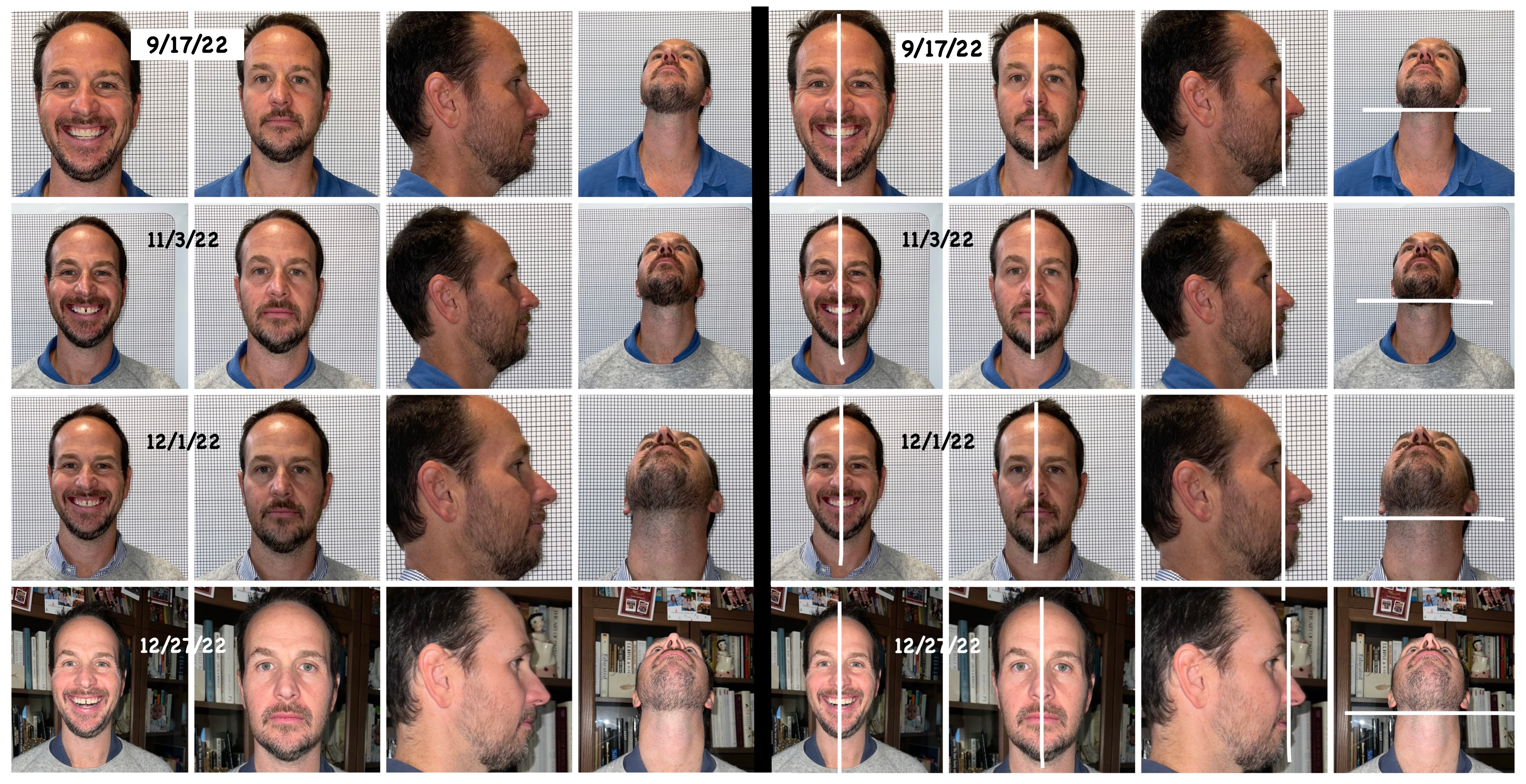
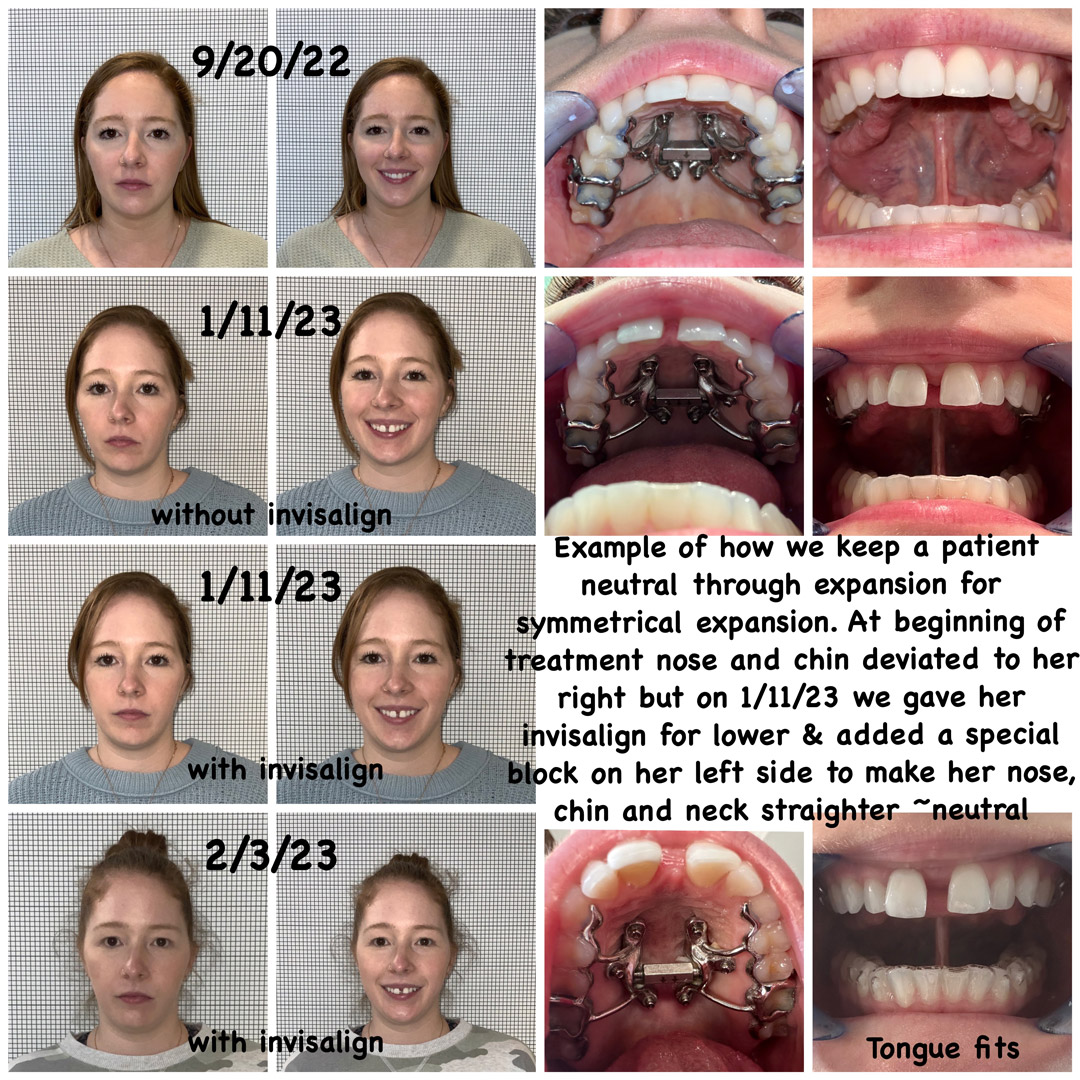
The collage above is an example of a patient during his MARPE journey. You can see how we have made his head more neutral and straighter and that his head is no longer tilted up, which he had to do as compensation to breathe better.

Why would a patient want miniscrews placed in the roof of their mouth for expansion?
- Any of the following patients should consider this kind of expansion:
- Any patient that cannot sleep through the night or does not wake up rested.
- Any patient with either sleep apnea or sleep-disordered breathing who has low Sp02 while sleeping.
- Any patient that always wakes up congested or is congested during the day and needs to breathe through the mouth at night or during the day.
- Any patient that always wakes up congested or is congested during the day and needs to breathe through the mouth at night or during the day.
- Any patient that has a deviated septum and constant sinus infections. Often, after MARPE, the septum is no longer an issue.
- Any patient that is a restless sleeper and is tired during the day.
- Any patient that has experienced nasal valve collapse and finds that Cottle’s maneuver allows them to get more air in. These patients usually like to use Breathe Right® strips, but often they do not open their nose enough.
- Any patient that needs to exercise with the mouth open because they cannot get enough air through the mouth.
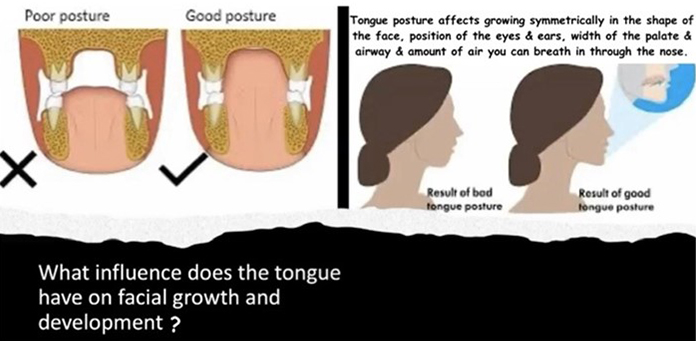
- Often patients are unable to park their tongue on the roof of their mouths because the tongue is too big.
- The goal is to fit the tongue on the roof of the mouth so it does not fall back into the airway during sleep.
- The top of the mouth is the floor of the nose. So, when we expand the upper arch, the patient has a much bigger airway through the nose. Many patients use reverse-pull facemasks to bring the upper jaw forward, which can provide anterior-posterior growth versus just transverse growth, and this is a whole lot easier than maxilla-mandibular advancement surgery (MMA).
- We know that if the roof of the mouth is wide enough, the tongue can be parked in the roof of the mouth and will have a home. If the tongue has room to fit in the roof of the mouth, this makes it more unlikely for it to drop back into the airway.
- Getting the expansion will help enable the tongue to be parked on the roof of the mouth. Since opening your mouth will not be needed if your tongue is parked of the roof of the mouth, this will also help increase nasal breathing.
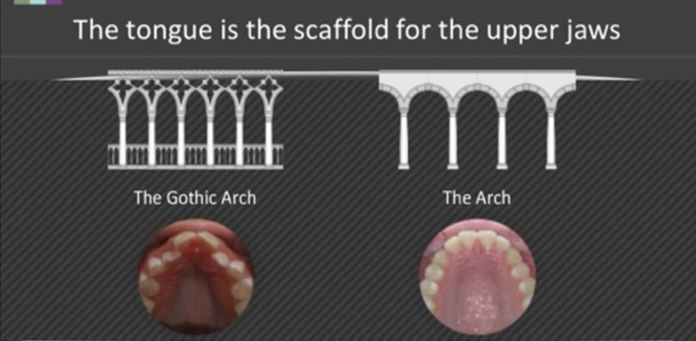
Comparison of Different Palate Shapes and Their Nasal Volume
The blue box represents the nose. Remember that the top of the mouth is the floor of the nose and that you can receive more air and breathe better with palate expansion.

How does Arlington Smile Center approach expansion in adults?
We consider the following questions:- How narrow is the roof of mouth and how close is the tongue to fitting in the palate?
- Does that patient have a crossbite that is going to prevent us getting their neck neutral to open up the airway?
- What is the patient’s chief complaint? For example:
- How congested are they?
- How bad is their sleep?
- Did they test with high scores of sleep apnea?
- Have they tried a CPAP machine?
Every patient is at a different point of their journey. We do not believe in a one-size-fits-all approach, as treatment really depends on what each patient brings to the table, and we discuss and weigh the best approach for that particular patient. Many patients want the quickest fix possible, and others would rather have a conservative approach. We honor each patient’s concerns and budget to get to the best solution to meet their needs. We will take a scan of their teeth and a CBCT 3D X-ray to look at the size of the airway, the size of tonsils and adenoids, and the position of the jaws. We will come up with a plan that meets the needs of each patient.
How we measure the width of the palate: Can the tongue fit?
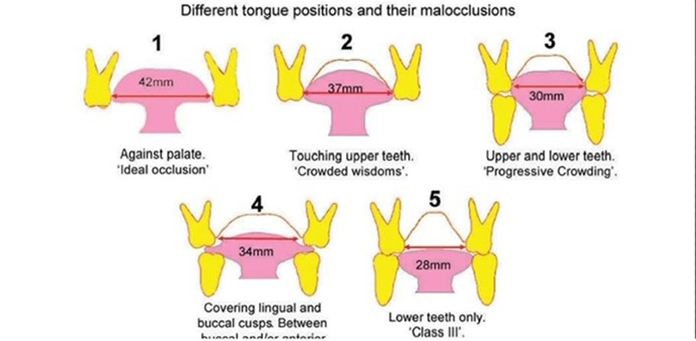
We measure the roof of the mouth. Original Transverse Measurement we denote as TM. We measure using the width of the mesial-lingual of tooth #3 at the gumline to the mesial-lingual of tooth #14 at the gumline across the width of the palate.Ideal Transverse Measurement (width of the roof of the mouth from first molar to first molar) is 45 mm for men and 40 for women. This width normally gives enough room for wisdom teeth to erupt into the mouth and allows for maximum opening of the palate. Since the roof of the mouth is also the floor of the nose, the Ideal Transverse Measurement also gives us increased room for nasal and pharyngeal airways.By age 4, ideally we want to see at least 30 mm, and by 6 years old, we hope to measure more than 35 mm. By 12 years old, we would love to see 40, and by 18 years old, 45 mm. Normally, if the patient is not at 35 mm by 6 years old and their tongue cannot fit in the roof of the mouth, we will not be able to get to anything higher than what they were at 6. This is because the tongue is what is expanding the palate. It needs to fit passively inside the teeth, not overlap the teeth, and the patient needs to learn to keep tongue suctioned to the roof of the mouth. Otherwise, the expansion will not stay expanded and the palate will get smaller and narrower over time.



MARPE is not limited to adults. We have also seen children experience amazing results with MARPE.
HOW EARLY SHOULD WE DO MARPE IN CHILDREN?
What ages are best for MARPE (miniscrew-assisted rapid palatal expander) vs. RRE (rapid palatal expander)?
Narrow upper jaw, or maxillary transverse deficiency, is an orthodontic problem that is prevalent in all ages. Children and young teenagers can have this problem fixed with a palatal expander due to their upper jaws not being completely fused in the middle. However, for older teenagers and adults, a palatal expander will often result in the back teeth sticking out instead of the desired jaw expansion.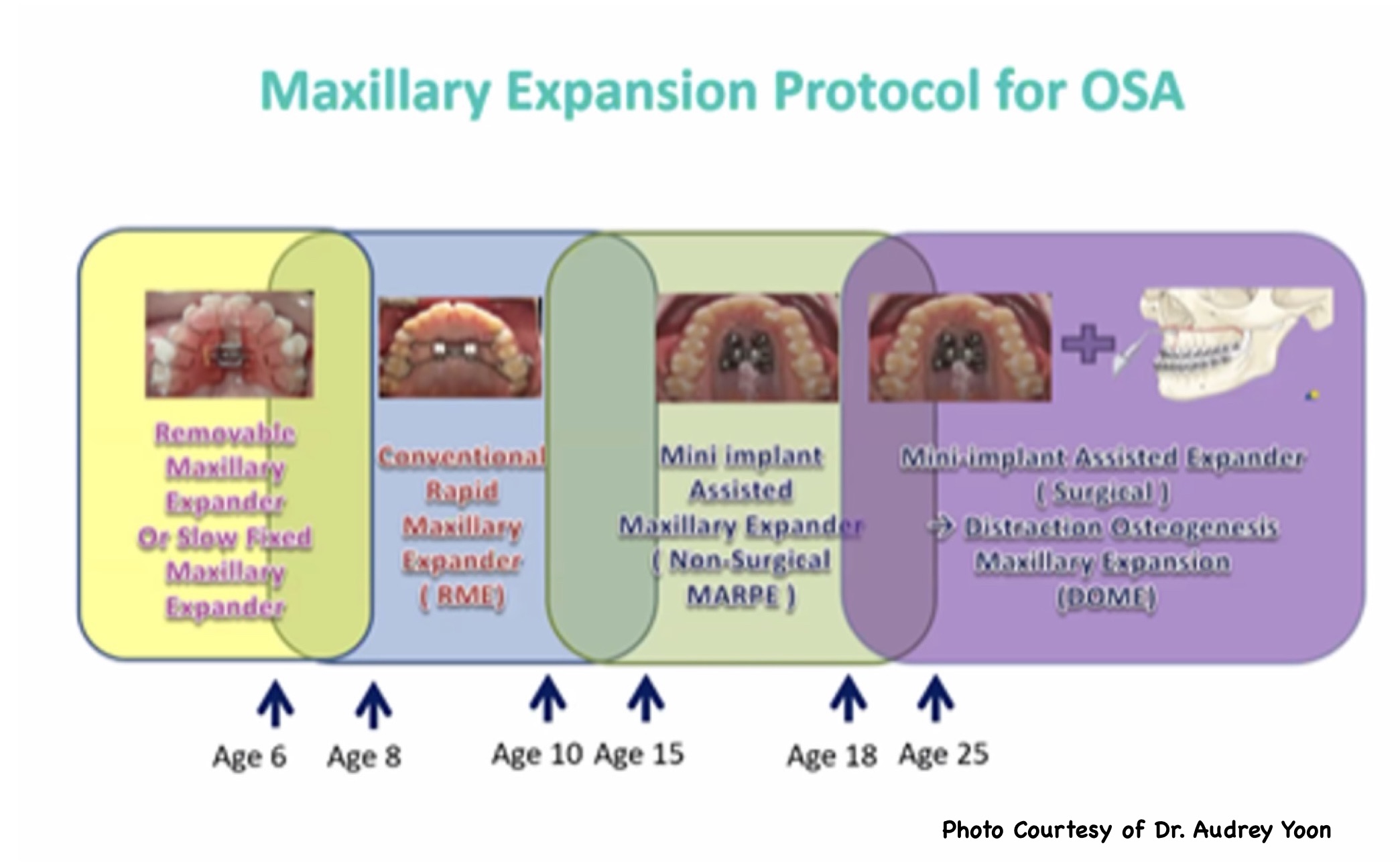
Why should my 10-year-old get a MARPE vs. a RPE?
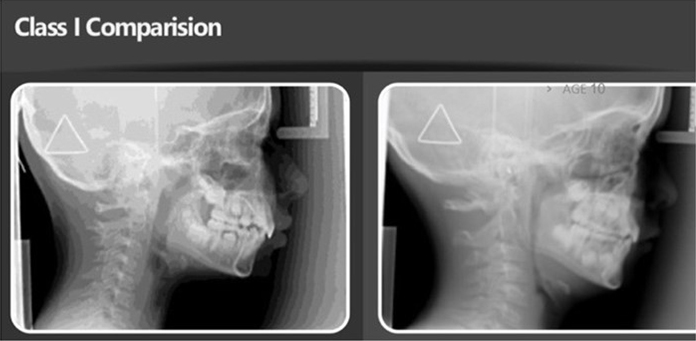
The bottom line is that we want their expansion to last and not collapse, and if we do MARPE, we have a much better chance for the expansion to last throughout their life. The photo below explains the difference and why we have so much more success with MARPE.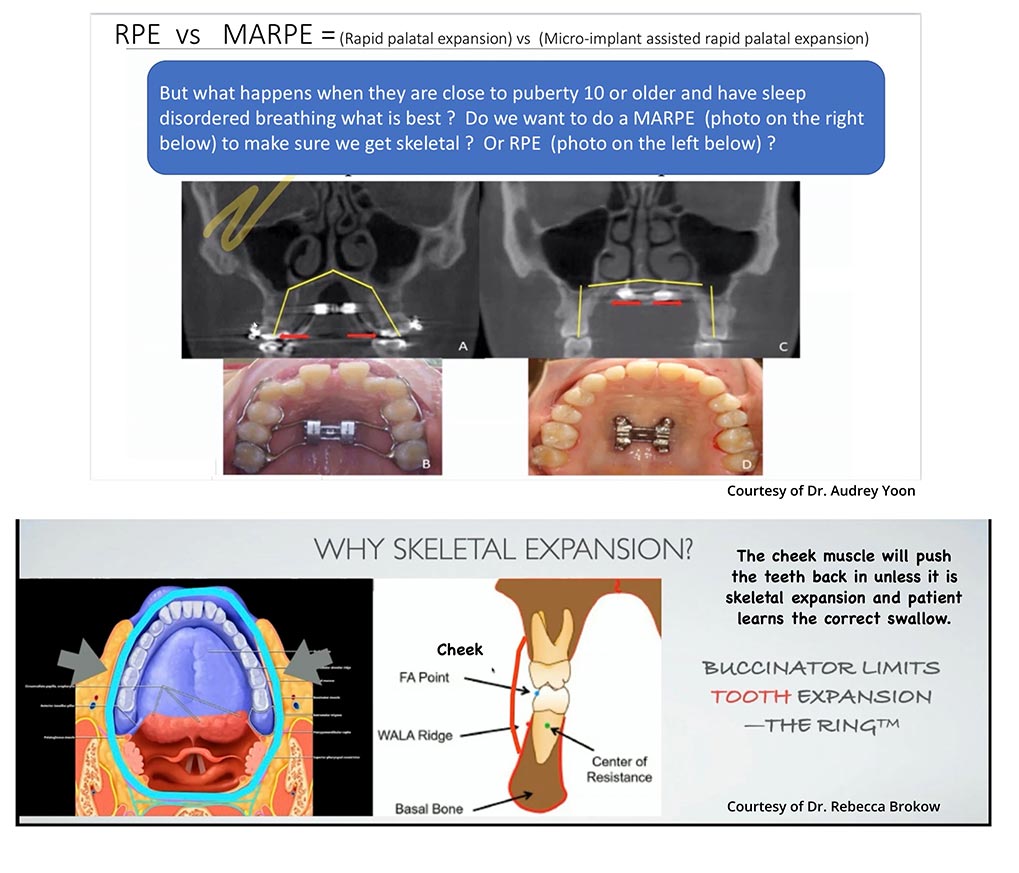
The graphics above help show the importance of skeletal expansion. If the child is older and has sleep-disordered breathing, often skeletal expansion is the way to go because we need the expansion to last. If they are close to having all permanent teeth, we may just be getting dental expansion with the rapid palatal expander, which is why maxillary skeletal expansion is the smarter option. If it is just dental expansion, we are just moving teeth, and over time, as many adults know, all the expansion is lost and they need braces all over again. But with skeletal expansion, we have a much better chance to keep the teeth from falling back and making a narrow palate all over again.
Research Showing the Effect on Children With RPE vs. MARPE
 We need to get the expansion and crossbite corrected early to avoid asymmetrical jaw growth.
We need to get the expansion and crossbite corrected early to avoid asymmetrical jaw growth.Dr. Rebecca Brokow cites the following conclusions:
Mandibular Asymmetrical Growth Can Be Secondary to Postural and Muscular Habits Early in Development
- Mandibular growth is restricted on the side of the crossbite, leading to a relative shortening of the ramus height and subsequent development of mandibular and facial asymmetry.
- Asymmetrical muscular potentials have been shown using electromyography in patients with crossbite — these neuromuscular patterns may persist after the occlusal contacts are eliminated.
- The presence of a unilateral crossbite is associated with a variable chewing patterns and large lateral deviation during closure.
- Uncorrected lateral crossbite can lead to increased asymmetry in the tempero-mandibular joints and in the condylar paths.
Kurol J. et al., 1992; Thilander B. et al., 1984; Linder A. et al., 1989; Cheng M-C, 1988; Ingervall B et al., 1975; Hamerling K., 1991; Schmid W., 1991; Haralabakis V., 1964; Troelstrup B., 1970; Moss, JP, 1980; Keeling SD, 1991; Myers DR, 1980; Pirttiniemi P. et al. 1994
Why is it so important that the patient’s crossbite is corrected?
When a patient has a crossbite, they cannot slide their teeth around to chew without their neck and airway being locked up. Also, a crossbite leads to asymmetrical growth in children.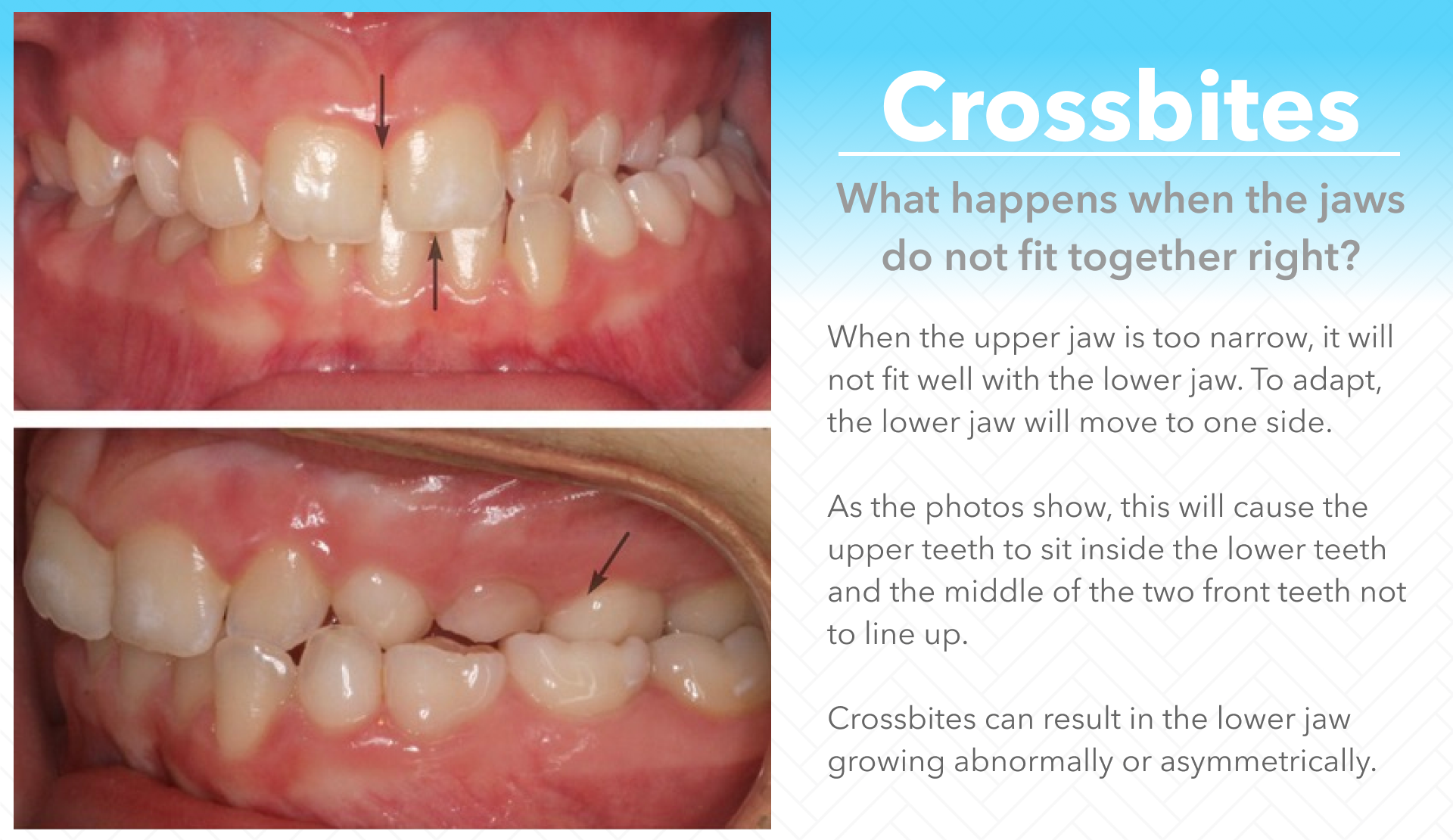
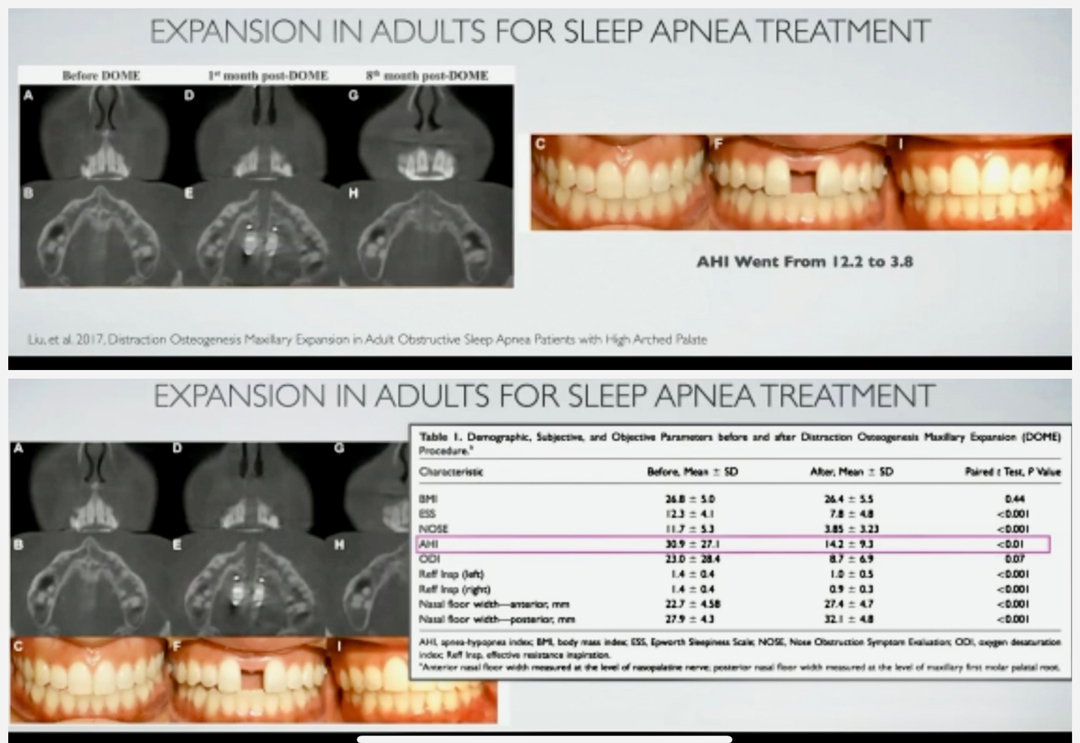
Research Showing How Effective MARPE Is in Reducing Sleep Apnea
 Dr. Roca orders radiology reports on every CBCT to check for the size of the adenoid and tonsils, size of the airway and health of the TMJ. It is particularly useful when the radiologist measures the jaw heights and shows that one side has a different ramus height than the other side. The radiologist often picks up torsion in the cranial sutures as well.
Dr. Roca orders radiology reports on every CBCT to check for the size of the adenoid and tonsils, size of the airway and health of the TMJ. It is particularly useful when the radiologist measures the jaw heights and shows that one side has a different ramus height than the other side. The radiologist often picks up torsion in the cranial sutures as well.What do we notice when patients have one ramus longer than the other?
A research study performed by Ho-Jin Kim, Mihee Hong and Hyo-Sang Park found the following:- “On deviated side, canines tipped buccally in maxilla and lingually in mandible.
- On nondeviated side, maxillary molars and mandibular canines extruded vertically.
- On nondeviated side, molars tipped lingually in maxilla and buccally in mandible.
- Dental compensation was associated with skeletal variables of deviated mandible.”
For additional information, refer to the following study.
Mechanobehavior and mandibular ramus length in different facial phenotypesThe following videos below were made by one of the respected MARPE mentors of Dr. Roca, Dr. Audrey Yoon
Here are additional resources:
For additional information, refer to the following study.
Create a Comparison of skeletal maxillary transverse deficiency treated by microimplant-assisted rapid palatal expansion and tooth-borne expansion during the post-pubertal growth spurt stage: A prospective cone beam computed tomography studycommon questions in reference to marpe/mse treatment
*These answers are subject to change as we discover better solutions
How do you decide what age to have MARPE/MSE treatment on male and female patients? What is the minimum age of the patient we can start MARPE/MSE?
If you are a child that is very narrow and has sleep disordered breathing that is affecting their well being I will do MSE if patients wish as early as age 6. But normally MARPE/MSE Is my go to expansion if child is 10-13. I will discuss pros and cons of other options and we decide together.
What are your age requirements for corticopunctures?
All males 25 or older and female over age 30, I use the Piezotome cube instead of corticopuntures Thin bone is an automatic customization and piezo for me. Thick bone w bicortical engagement is a good thing and if patient prefers and female I will try without Piezo if they prefer. Male over 25 needs to get Piezo.
Are there age limitations with utilizing a Reverse pull face mask with MARPE/MSE? How much do you gain of forward growth?
Age is not the deciding factor. MSE is useful for young patients with
- High angle
- Midfacial deficiency that required bone-borne protraction
- Nasal airway obstruction
- Class 3 occlusion
- Bimax retrusive
- Narrow maxilla
- Wider width of mandible
We consistently get more than 8 mm protraction with good cooperation in growing patients. We have observed about 3-5 mm in mature patients
Sometimes the patient’s Palatal vault is so narrow that even 8mm MARPE/MSE cannot reach the palate. What do we do for these patients? How do we adapt MSE to severely constricted maxillary arch?
Often I need to use another MARPE design like a superscrew for initial expansion and switch over to MSE as a second expander if second expander is needed for more expansion.
What is the minimum bone thickness you’re looking for to place the implants?
The posterior bone is often thinner than 5 mm but still works most of the time. Other factors should be considered as well…bone density, bone morphology, special relationship between force vector and resisting structures, We use Partners dental studio that merges our CBCT with the intraoral scan of their mouth with their software to make a custom design placing the tads exactly where we will have enough bone. Some tads are shorter some are longer just to make sure we get bicortical engagement which we know we will since they use this software to get us precision removes all guesswork.
Do you place spacers before installing the MARPE/MSE?
No we use 3D printed bands that sit on top of the molars so we do not need to add spacers before we place the MSE
What happens when the bone is very thin in the posterior area in some patients? Is there any risk?
Yes, it may not work. We will try to design a custom marpe for this patient and we can try, I have seen thin bone work many times. Many doctors had a higher failure rate with thin bone which is why we cose to do always custom MARPE. We have become pretty creative with our designs since using this software sometimes if the entire palatal bone is thin, I use the lateral implants with or without acrylic pads.
During the insertion and penetration of the second layer of cortical bone, are you not worried about penetrating the nasal mucosa?
Now that we are using the software with Partners dental studio we know that we are only penetrating 1 mm beyond bicortical so I can confidently say this is not an issue. However in the past before the software this could happen with no negative consequences.
Can we use this in patients with pain from Temporomandibular Joint Disorders?
I prefer to do MSE in patients with inactive TMJ, although others have used MSE as a TMJ treatment modality. I have done personally and the TMJ improved but it is really on a case by case decision.
If you had a patient that you wanted to minimize widening of nasal alar base, would you not want to use MARPE?
Any expander that produces a V-shape expansion will widen the nasal alar base. Since MSE produces a parallel expansion, it is less of a concern. But patients should not be doing MARPE case for cosmetic reasons. I always tell patients if you do not like how the nose is looking we can always turn backwards. It is reversible if we do not allow suture to fuse.
Can you elaborate more on how to fabricate MARPE on patient with canted palate?
Position the jackscrew perpendicular to the septum rather than adapting it to the canted palatal vault. But now that we have the software we can angle the lumen where the tad enters in different angles and depths to correct the canted palate in the custom designed MSE/ Marpe
Treatment questions:
What are your turning protocols ?
In children after placing the MSE, I wait 1 week and start turning and start using the reverse pull face mask, followed by one turn a day until it splits. After it splits we turn every day for 2 to 3 weeks and if wearing a face mask we go to 3 turns a week. Adults is the same but we start the turns the day we place in mouth turning 4 times followed by once a day.
Will the patient feel tingling or sneezing in all screw insertions or just the first one?
Only when it is through the second cortical layer… but often the patient may not feel anything. If we use a lot of anesthesia nothing is felt.
What home sleep test are you using?
We use a sleep image ring that you can learn more about at Sleepimage.com It is FDA approved to check for sleep apnea in children over 2 and adults. We use it to give us a baseline to start and we can repeat after three months of starting treatment. It is inexpensive and easy but nothing is as good as a sleep lab. We own the ring and you borrow it and just pay for the reports. This allows more than one night to give us more accurate results in case you have a bad night……and it makes it easy to test throughout treatment to see positive rerduction in fragmented sleep and apneas.
Do you need to do any kind of Pre-drill?
Yes, before placing the tads we use a pilot drill that is the same size as the lumen so that we are assured correct angle placement of the tad since the tad is more narrow than the lumen it allows easy access direct to the pre-drill hole when we enter with the tad.
Why is it necessary to put two additional mini screws?
They promote parallel expansion, and having four reduces the strain per implant during the expansion. Sometimes due to age or thickness of bone we will add more tads. It is on a case by case basis. .
When do you start to close the diastema between two front teeth ? What about the concerns of roots of central incisors moving into the expansion space before new bone development?
One theory is that there is bone on the medial side of the roots…no different than retracting the canines into the extraction site immediately after extracting bicuspids…taking advantage of the regional acceleratory phenomenon (RAP). Another theory is to wait for 2 months once you stop turning the upper to start closing space. The options will be discussed with patients.
What happens to the Vomer bone after expansion?
Vomer is a very thin bone housed inside fibrotic sheets. As the hemifacial structure rotates downwards and outwards, the vomer moves inferiorly little. It generally stays within the sheets which splits at the bottom as the PNS split.
How often do we see the patient after insertion?
The child patient I like to see one week post op to be the one to turn it for the first time and introduce the reverse pull facemask. After that I see everyone every 4 weeks. However, every Sunday Dr Roca likes the patient to text her photos of the marpe expansion, bite, and diastema directly to my cell phone.
In case you have large palatal tori, did you use corticopuncture? If yes, how?
Yes if you have a large tori it makes no difference we just go deeper in that area with the piezotome.
Can you do MARPE/MSE if you have posterior implants (unilaterally)?
We are not moving teeth we are opening the bone in the suture so it would not change anything. You may however need to replace the crown on the implant after Invisalign is complete so the new crown fits properly into the bite. The only problem occurs if you have anterior implants we will not be able to close the space with Invisalign and we need to get very creative how to handle this hurdle.
Any precaution to be taken while dealing with a patient with Nasal Septal Deviation?
I recommend waiting till after the MARPE/MSE is finished to see how the breathing is feeling and after that you may want to correct the deviation if it is bothering you. We have never made nasal deviation worse up to now but often remove the need for surgery.
What are your recommendations for asymmetric expansion in young patients?
Every expansion with any device is asymmetric. No one is symmetric and reciprocal force will produce asymmetric expansion. It is difficult to predict which way the expansion will go because there are too many variables involved. However, the best way to encourage symmetric expansion during any treatment is with routine work with the Posture restoration Institute (PRI) – Physical therapist or cranial osteopathic physician that help us keep your cranial sutures loose to promote symmetric expansion.
How many months are expected for retention after active expansion?
We cut off the arms to the MSE and Leave the jackscrew with implants for 6 months but start the orthodontic treatment immediately.
What is the anterior/posterior position changes in midfacial segment after expansion?
The midfacial structure rotates forward with the fulcrums near TMJ area.
Why do some doctors turn several times a day and more rapidly than you do?
Everyone has studied with different mentors and finds what works best in our hands and with their patient pool.
Do patients that have had nasal septal correction surgery present a problem for opening the suture?
We were able to do it with no problems.
What protractors would you recommend for each age group? From 5 year old to teens adults etc?
Any facemask will work we give you one included with your treatment but you can purchase others if you prefer another one.
What would be the force/duration recommendations for Facemask with MARPE/MSE?
About 500g each side for growing patients…but 500-1,000g for mature patients.
How do you know MARPE/MSE has failed?
Dr. Roca has not had an MARPE or MSE fail but it does happen. Since Dr Roca uses the Piezotome in her adult cases she has never had one fail and does not expect one with the intense custom planning she does for every case. She has found working so closely with the lab that uses the software to merge the CBCT with intraoral scan of the teeth we can prevent failures. However, since adult skeletal expansion is not a natural process we never know on each patient what will happen. If the patient does not have a space between their front teeth, what we call a “split by 3 weeks time – we check TADs. If they are not tipped we keep going for one more week. If still does not open we will take a new CBCT to check. If position or the TADs is good but it failed – usually because the placement is too posterior in a thin bone – we turn all the way back and remove the remove MSE, let tissue heal and do a piezo if it was not done or remake the MSE and move it either more forward position or add extra custom TADs. Again, with all our planning, Arlington Smile Center track record is all cases have split.
How often should we take progress CBCT or frontal?
I like to limit xrays whenever possible so I will not order a new CBCT unless the patient wants one or treatment dictates that I need a new one. However, throughout the process I take one small periapical xray of the two front teeth to track the split.
Age limit for MARPE/MSE? What is the oldest age recommended?
My mentor, Dr Lipkin had a 64-year-old male… now using the piezotome much easier. My oldest has been a 56 year old female and 54 year old male.
Can we attach the supporting arms to dental implants?
Can we attach the supporting arms to dental implants?
What are the effects of MARPE/MSE on TMJ?
I have yet to see any negative consequences yet but it is bound to happen.
Is the MSE/MARPE rigid arm model used in patients with a face mask?
We usually use the soft arms on the MSE cases but more rigid arms on the custom MARPE cases.
One side is insufficient expansion while the other side is over expansion, what should we do?
One option is to cut off the arms on the over-expanded side and compensate or add a turbo (composite resin filling) on the lower molar of the side that has not expanded to unlock the sphenoid and temporal bone.
In the case of using face mask, do we need to have a different consideration with the force we apply?
Expansion force will be the same. Protraction force can be anything since any force is orthopedic (it is a bone-borne protraction). Heavier force and longer duration are more efficient.
With Reverse Pull Face Mask is it best to add protraction after transverse is complete? Or simultaneously? And, for how long? And, are you utilizing this for A-P deficient patients in addition to Class III?
Simultaneous protraction is better; 14+ hours will produce a great result (it has to be more than 10 for any positive progress); I do not like to use Class III elastic (it causes lower dental compensation) if patient is a good cooperator with Face Mask.; Face mask protraction promotes a forward and downward movement of maxilla; Class III elastic tends to rotate the maxilla in a counterclockwise direction (not good for a high angle case).
Should we straighten our teeth before MARPE/MSE? Or can it be placed on rotated teeth (molars)?
I prefer to expand first and then de-rotate after cutting off the arms. You can also band another tooth. we have found it does not matter so much which teeth you band as long as you have one band on the first or second molar.
How long do you leave the MARPE/MSE in after expansion is completed? How soon can you start orthodontics? How long do you leave MARPE/MSE in for Class III protraction?
We leave MARPE in for 6 month after completing the expansion; if protraction case we leave in usually for 8 months. Sometimes I leave MARPE it in place and use it as an anchorage for various tooth movements.
No limit on older patients for MSE?
Generally harder as we go beyond late 20’s (male) but age is not the only factor. I have successfully treated many older patients. Using Piezotome with every patient is the way to go to increase success.
How do I know if the MARPE/MSE isn’t working (no arm bending, no screw breakage) no diastema alone or with other presentations?
You see the implants severely tipping or cutting through the cortical bone, the jackscrew falling apart, the arms bending and impinging against the tissue, etc. The screw not advancing.
When closing the diastema, how do you not collapse or lose any of the oral volume space that was created?
With expansion, the midfacial structure moves anteriorly with a larger overjet. Generally, the original incisor position is recaptured after the space closure; however, the oral volume is gained by the increase in width. If the incisor position after the expansion is desired to be the final position, then you can cut off the arms and protract to the entire arch…but this will be a rare instance.
What is the optimal expansion protocol, can you elaborate with more detail please?
The limiting factor is the lower arch. You can expand the upper basal bone as much as required to accommodate for lower decompensation and tongue space. Most of the time, the lower jaw is not narrow but the dental arch is because of the lingually collapsed lower posterior teeth. BEFORE, I would estimate the projected lower buccal surface (after the decompensation) by taking the width from the buccal points adjacent to the furcation of lower first molars. I expand until the narrowest area above the maxillary first molars becomes wider than the estimated lower buccal surface. This allows a full decompensation of both upper and lower posterior teeth. However, in very narrow upper arches with not enough buccal bone of the lower teeth we will need to stop expansion when the lower molars are uprighted or we will need to SFOT. NOW, Invisalign has a new feature that allows us to merge the CBCT 3d xray data with the scan of the teeth so there is no more guessing we know exactly how much we can expand each lower tooth. This new feature has really decreased the need for SFOT.
Watch this video I prepared that explains this.
What are my options if the expansion does not work?
While MARPE has a high success rate, its success is dependent on several factors which include your ageand bone density. We cannot guarantee that the MARPE will be a success, and we have alternative options that we can propose if the MARPE does not work.
What are possible complications and risks with MARPE/MSE?
I have heard that there is a rare chance of optic nerve complications / changes in vision with this type of expansion. Is this true, and if so, have you experienced such complications?
Dr Moon did an extensive optic study and found that No functional change was observed. The optic nerve comes through a part of sphenoid bone, and an expansion has no impact whatsoever.
Failure of midpalatal suture to split
Always a possibility but we know how to avoid this.
Discomfort due to adjustment and application of MARPE
Usually lasts for 5 days.
Swelling, infection, bleeding, and/or pain at the site of mini-implant placement
This can happen at anytine during the process but we normally only see this in the first week if piezo was done, we just avoid it by giving antibiotics to prevent infection if Piezo procedure is used.
Congestion, sinusitis, and/or tingling sensation in the nasal and sinus area
This can happen as the MARPE expands everyone reacts differently usually we see improvement in breathing within a couple weeks.
Failure of the implant to take hold
Mini screw might unravel and we may need to take it out.
Allergic reaction to anesthesia and/or orthodontic materials
We do not like to do a marpe on a Patient allergic to metal or nickel to avoid this complication.
Loss of teeth vitality
If a tooth is not healthy before the MARPE is placed we can not control what happens during treatment which is why Dr Roca tests all teeth before she places marpe.
Although rare, temporary hearing loss, paresthesia, numbness, and/or loss of sensation
Dr. Roca has never seen this in her patients but it has been found but in older patients
Asymmetric expansion or unfavorable facial changes
we watch this very carefully and go very slow so we can always reverse turn if necessary. We work closely with the PRI (physical therapist) to avoid assymnetry.
Lastly it is important to know if the MARPE does not work additional treatment may be required due to unforeseen circumstances or inability of midpalatal suture to split (e.g. orthognathic surgery)